PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2019) Volume 6, Issue 5

Author(s): Sorabh Augstam*and Parminder Singh
Clinical-Medical Image:
A 32-year-old male, labourer presented in cardiology department with progressively increasing easy fatigability, distension of abdomen and
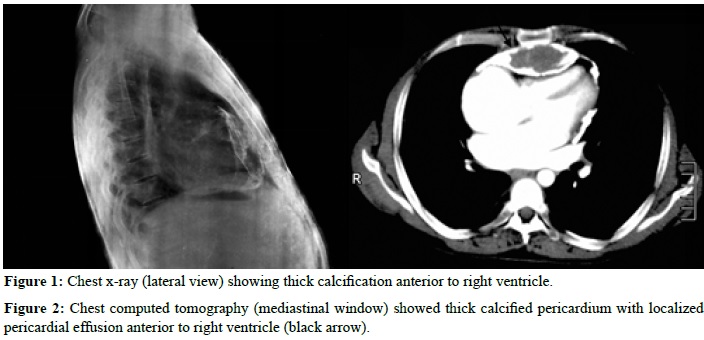
pedal edema since two years. He had past history of pulmonary tuberculosis three year back for which he had taken 6 months of antitubercular regimen under DOTS. At time of presentation, heart rate was 90 bpm, rest of the vitals were normal. Jugular venous pressure was raised 6 cm above angle of louis with prominent X and Y descent. Bilateral pitting edema was noted. Pericardial knock was appreciated on cardiac auscultation. Chest x-ray showed calcification anterior to right ventricle (Figure 1). Echocardiography showed mild pericardial effusion with thick parietal pericardium and septal bounce. Computed tomography showed thick calcified parietal pericardium with localized pericardial effusion anterior to right ventricle (Figure 2). Patient was investigated for reactivation of tuberculosis; however there was no evidence of it. Patient was started on diuretics and is planned for pericardiectomy. Chronic constrictive pericarditis is long-term inflammation of the pericardium. The pericardium is the sac-like membrane that surrounds the heart. Inflammation in this part of the heart causes scarring, thickening, and sometimes calcification.
 Awards Nomination
Awards Nomination