PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical Image - International Journal of Clinical & Medical Images (2018) Volume 5, Issue 6

Author(s): Sanne De Smet
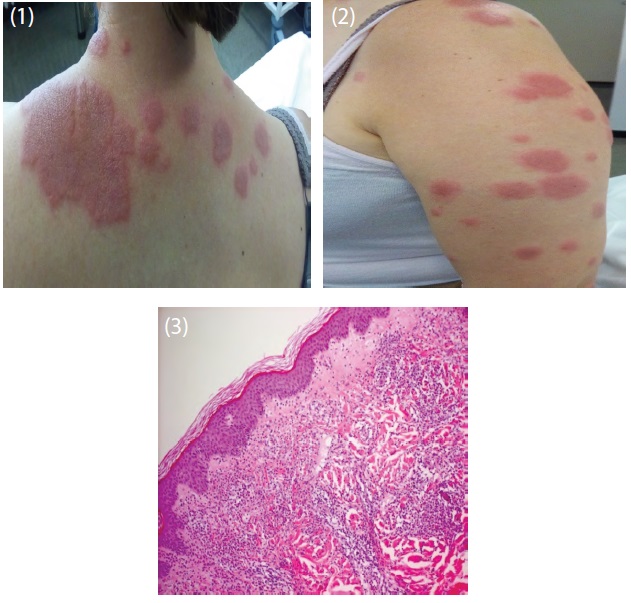
At the emergency department a 42-year old women presented with a rapidly progressive skin disorder. It started a few days earlier with a small plaque on the neck, spreading quickly to the thorax, abdomen and both legs; accompanied by fever. She had no significant medical history and took no medication. 3 weeks before she had complaints of an upper respiratory airway infection (Figures 1 and 2). Lab results were normal, besides a mild thrombocytosis and a high CRP of 250 mg/dL. The lesions could be described as sharp-edged, slightly elevated erythematous plaques and looked like those seen in sweet syndrome (or acute febrile neutrophilic dermatosis). A biopsy is one of the lesions showed a neutrophilic dermatosis without leukocytoclastic vasculitis, compatible with Sweet Syndrome. Therefore oral corticoid therapy was started with regression of the lesions after a few days (Figure 3). Sweet Syndrome is typically seen 1-3 weeks after respiratory/gastro-intestinal infections or is associated with (haematological) malignancies or auto-immune systemic disorders. Screening for haematological malignancies was done by performing a bone marrow aspirate and biopsy, but showed normal findings.
 Awards Nomination
Awards Nomination