PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical Image - International Journal of Clinical & Medical Images (2014) Volume 1, Issue 8

Author(s): Cyriac Abby Philips, Lovkesh Anand and K N Chandan Kumar
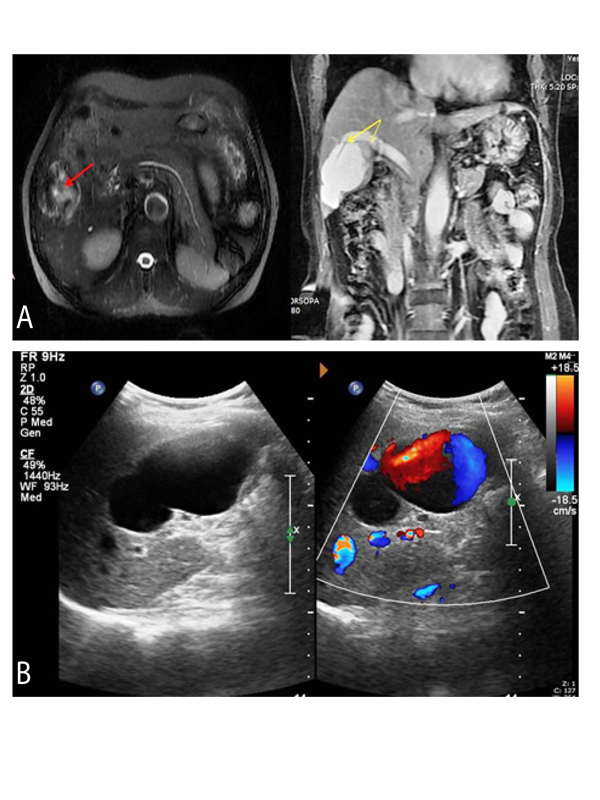
A 52 year old housewife with no known co-morbidities or addictions without prior history of hospitalizations presented to our outpatient department with complaints of dull aching pain in the right upper quadrant associated with nausea, in the absence of fever, jaundice, anorexia or abdominal distension. She denied menstrual irregularities, complementary or alternative medicine and contraceptive use. On examination, she was found to have a blood pressure of 128/60 mm of Hg in the supine right brachial region with tachycardia. Pallor, icterus, cyanosis, clubbing, adenopathy and peripheral edema was absent and the abdominal examination revealed mild tenderness in the right upper quadrant without organomegaly, ascites or bruits. The rest of the systemic examination was essentially normal. Her investigations revealed a normal hemogram with preserved liver function, renal function and normal pancreatic enzyme levels. An ultrasound of abdomen done at a center outside revealed an SOL in the right lobe of liver. She underwent a contrast MRI of the abdomen (Figure A) followed by an ultrasound Doppler of the liver (Figure B) for confirming the diagnosis. The abdominal MRI revealed a 5.8 x 5.6 x 4.5 cm well defined lobulated T1-hypointense and T2-hyperintense lesion in segment VI and V, subcapsular in location. T2WI showed multiple areas of flow voids within the lesion with heterogenous signal intensity (Figure A, red arrow). Post contrast studies revealed complete filling on venous phase which persisted in the equilibrium phase turning iso-intense on delayed hepatobiliary phase. The segment V branch of right portal vein showed the ‘luminal continuity’ sign (Figure A), yellow arrows]. Attendant multiple simple non-enhancing T1-hypointense and T2-hyperintense cystic lesions were seen in both lobes of liver. An ultrasound Doppler of the liver showed anechoic signal from the above lesion with color filling on Doppler and monophasic flow on pulsed Doppler (Figure B). Barzilai and Kleckner first reported a case of main PVA in 1956. PVA’s constitute 0.43% and 3% of all aneurysms and venous aneurysms respectively. A PV diameter more than 20 mm is diagnostic of aneurysm (average in healthy subjects 15mm; cirrhosis 19 mm). They are either congenital or acquired and extrahepatic (more common, commonest location MPV > splenomesenteric venous confluence) or intrahepatic (at bifurcations). The former occurs due to progressive enlargement of diverticular remnant of vitelline vein forming a saccular aneurysm later in life and the latter in cirrhosis, portal hypertension, pancreatitis, abdominal surgery, and trauma and in Osler Weber Rendu Syndrome. Presentation is mostly asymptomatic and complications include thrombosis, rupture, compression and portal hypertension. Medical management is by anticoagulation and surgical options include aneurysmorrhaphy, portocaval shunt, and mesocaval shunt. This case teaches that the initial evaluation of liver SOL must include a baseline color Doppler study for early diagnosis and resourceful management.
 Awards Nomination
Awards Nomination