Abstract: A 6-year-old male child presented with a discharging sinus on the left cheek 3 cm lateral to left oral commissure in our outpatient department. A provisional diagnosis of parotid fistula was considered. CT sinogram ruled out this diagnosis. Histopathology after excision showed it to be the first branchial cleft sinus.After extensive literature search, we found that this sinus was present at an abnormal location. The site of the sinus was out of the triangle described by Triglia where most of the first branchial cleft sinuses are located, hitherto unreported in world medical literature. Keywords: First branchial cleft sinus; Triangle of Triglia Introduction Otorhinolaryngologists commonly diagnose branchial cleft anamolies. Most of these anamolies are present in second branchial cleft. First branchial cleft anamolies form less than eight percent of these [1]. Due to rare presentation of first cleft anamolies, the diagnosis is generally delayed and treatment inappropriate [2]. The abnormal closure of ectodermal portion of the first branchial cleft is the reason for the formation of sinus, fistula or cysts in the neck. The locations of these anamolies are the most important key point in the diagnosis of these lesions. Most of these anamolies are present in the triangle described by Triglia [3]. We are hereby describing a case of first branchial sinus present outside this above described triangle, thus mimicking a congenital parotid fistula. This is a unique case reported for the first time at this site in English medical literature.
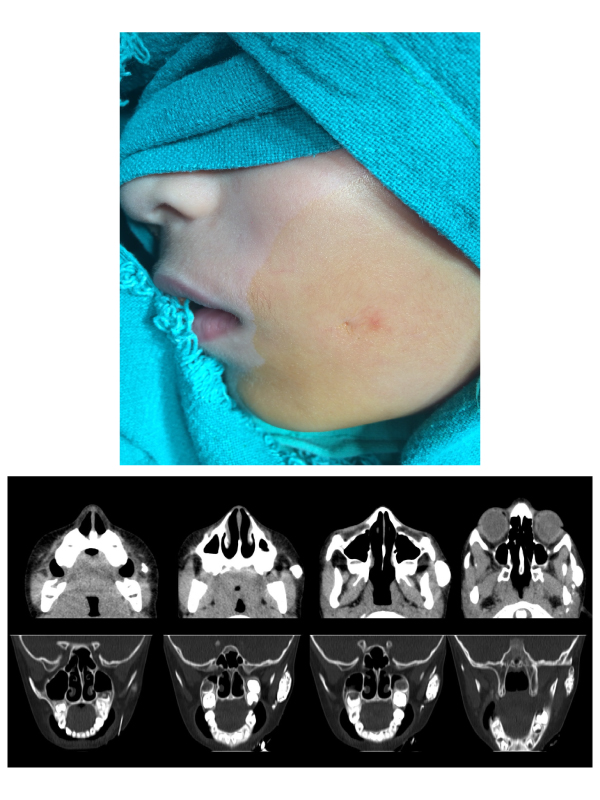
Case Report: A 6-year-old boy presented with a discharging pit in the left cheek since birth. There was no history of swelling, pain or any prior surgical intervention in that area. On examination, a cutaneous pit was seen 3 cm lateral to the left oral commissure (Figure 1). Clear watery discharge could be expressed from the opening. Surrounding skin was normal in colour. No other abnormality was detected in oral cavity, oropharynx and ear examination. Facial nerve function was normal. CT sinogram revealed the presence of a blind-ended contrast filled sinus of 4.3 mm caliber and 3.7 cm length extending superomedially in subcutaneous plane with terminal pooling of contrast lateral to ipsilateral masseter muscle. No communication with the parotid gland was seen. (Figure 2) Based on the clinical examination and CT findings the diagnosis of parotid fistula was ruled out. After taking written informed consent patient underwent a complete surgical excision of the sinus tract under general anaesthesia. Parotid tissue and facial nerve did not need any dissection. The postoperative period was uneventful. Histopathology report of the excised sinus was suggestive of an inflamed branchial sinus partially lined by pseudostratified ciliated columnar epithelium and partly by squamous epithelium with wall showing presence of chronic inflammation. Postoperative period was uneventful with no untoward complication or recurrence reported until date.
Discussion: First branchial arch anomalies have previously been sub-classified as aplasia, atresia, stenosis and duplication. Our case was a duplication anomaly. Typically, duplication anomalies demonstrate a normally developed external auditory canal along with a sinus tract extending from the external auditory canal to the skin of face or neck.
First branchial arch anomalies are often located close to the parotid gland, especially the superficial lobe that overlies the lesion. Its relationship with facial nerve is variable. The tract may run superficial to, deep to or in between the branches of the facial nerve. It is generally accepted that optimal treatment of these lesions is surgical with complete excision of the tract. In our case, the CT sinogram did not show any communication with parotid or facial nerve and hence these structures were not explored. This case posed a diagnostic dilemma due to its similarity to congenital parotid fistula [4,5], which itself is a very rare entity.
However, CT sinogram in our case showed no communication with parotid or any other salivary gland and there were no associated salivary cysts hence this diagnosis was ruled out. In a retrospective review of 39 cases by Triglia, it was observed that all patients’ cutaneous defects occurred within a triangle. The apex of the triangle was located at the external auditory meatus and its base as a line between the tip of the chin and middle of the hyoid bone. Its two-remainder sides curving from the external auditory meatus to the tip of the chin along the body of the mandible and from the greater cornu of the hyoid bone.3 In the present case, the cutaneous defect was present outside this triangle and first of this kind of case reported in medical literature. Most common complications after such excisions include infection, damage to the facial nerve and lower cranial nerves. Recurrence rates vary from 3% in primary cases to 20% in revision cases [6]. However, patient is fine after 2 years of surgery without any recurrence and is on regular follow up. To conclude, we recommend keeping first branchial cleft anamoly to be considered in differential diagnosis at the location of cheek also. CT sonogram is very useful investigation in these cases.



 Awards Nomination
Awards Nomination