PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2014) Volume 1, Issue 8

Author(s): Faisal Siddiqui, Mary Carter and Susanti Ie
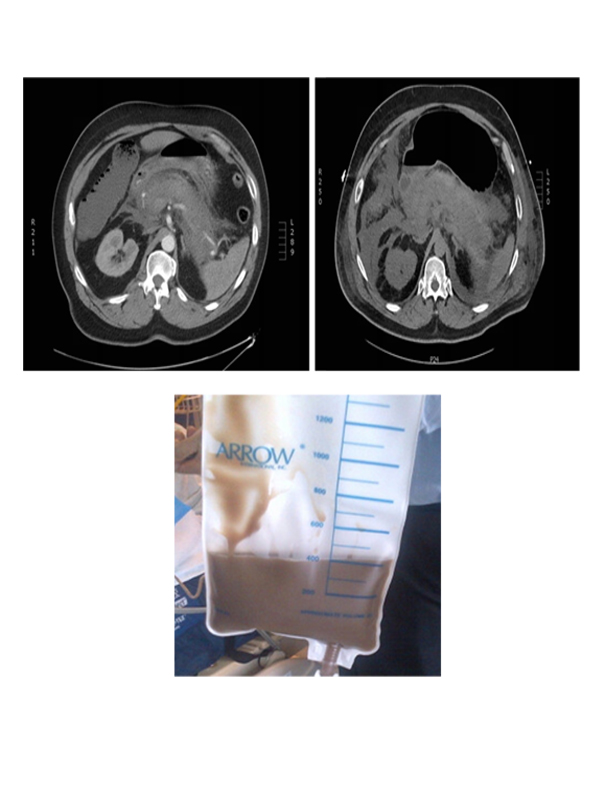
While Hypertriglyceridemia is recognized as the third leading cause of acute pancreatitis and is found in 12-38% of all the patients with acute pancreatitis [1]. But is rarely seen when the triglycerides are less than 20 mmol/L [2]. We present here a case of 54 year old male with past medical history significant for diabetes, hypertension and hypertriglyceridemia who presented with abdominal pain. He was diagnosed with acute pancreatitis on admission on the basis of biochemical and radiological evidences (Figure 1). There was no history of recent alcohol use or biliary pathology on admission. His triglyceride level on admission was 1681 mg/dl (19.1 mmol/l). During the course of his stay in the hospital he developed severe hemorrhagic pancreatitis (Figure 2) and multi-organ failure. He required endoscopic drainage of the peri-pancreatic fluid and also paracentesis that revealed brown colored ascitic fluid (Figure 3). He was continued on organ support, broad spectrum antibiotics, intra venous insulin and heparin therapy. He eventually recovered and was then transferred to the general medical floor. Learning Objectives: 1. Always consider triglyceridemia as a cause of pancreatitis even when triglycerides are less than 20mmol/l. As prompt therapy with insulin and heparin infusion can lower the triglyceride level and improve outcomes. Figure 1: Some inflammatory stranding and fluid around pancreas consistent with acute pancreatitis Figure 2: Severe Hemorrhagic pancreatitis with abdominal fluid collection. Figure 3: Brown colored ascitic fluid.
 Awards Nomination
Awards Nomination