PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2016) Volume 3, Issue 5

Author(s): Slama Iskander, Hidoud Amar, Jouve Bernard, Quilici Jacques, Boudes Audrey and D
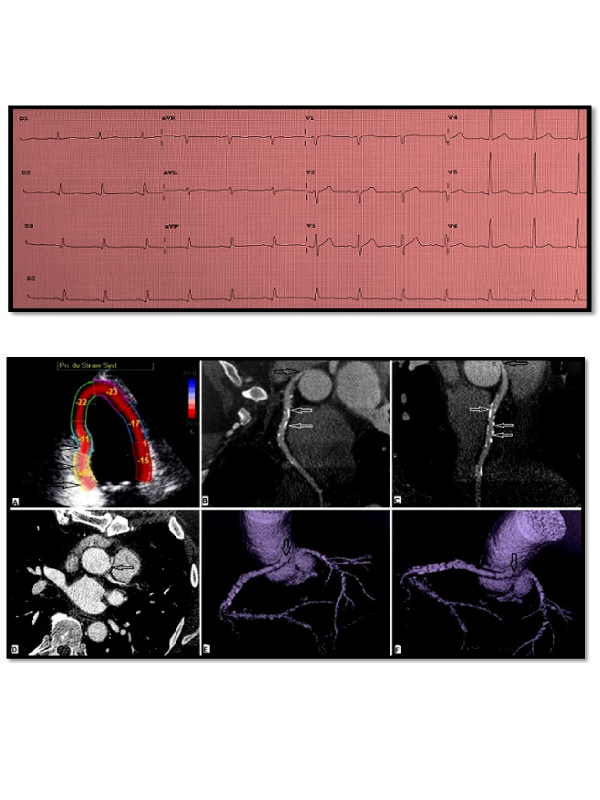
Case presentation: A 46-year-old male was referred to the echo laboratory for further investigations of a 6-months history with typical chest pain that is predictably exertional. His past medical history was largely unremarkable and so was his cardiac physical examination. Electrocardiogram showed sinus rhythm, poor R wave progression in anterior precordial leads and small Q waves with isoelectric T waves in inferior leads (Figure 1). Transthoracic echocardiography revealed prominent basal inferior and mid inferior hypokinesis with reduced regional myocardial longitudinal strain (-9% and -11% respectively) (Figure 2A). Left ventricular ejection fraction was estimated to be 50%. Myocardial perfusion scintigraphy was positive for a significant reversible stress-induced ischemia of the inferior wall. Coronary angiography showed normal left coronary system and anomalous origin of the right coronary artery (RCA). For further assessment, ECG-gated cardiac CT angiography (CTCA) was done and revealed RCA arising from left aortic sinus separately of left coronary artery, with inter-aorto-pulmonary course and ostial-post-ostial part severe luminal narrowing at the takeoff portion (Figures 2B-2F), coronary artery calcifications of the mid-RCA without significant stenosis (Figures 2B and 2C) and no significant atherosclerotic disease of left coronary system.
Surgical treatment was required. In fact, aggressive surgical management is often recommended to avoid sudden cardiac death, especially in documented coronary ischemia as a result of a coronary compression when coursing between the great arteries. The CTCA has an incontestable place as a first imaging modality tool for the assessment of the origin and course of coronary arteries and the detection of inter-aortopulmonary course that implies an appropriate surgical management.
 Awards Nomination
Awards Nomination