PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2020) Volume 7, Issue 5

Author(s): Tony Ete, Amit Malviya, Manish Kapoor, Vanlalmalsawmdawngliana Fanai, Shakeel Ahamad Khan and Animesh Mishra*
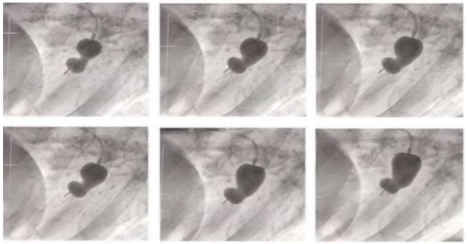
A 35-year-old female got admitted with complaints of breathing difficulty on exertion for 6 months. She also complained of associated swelling of both lower limbs. The patient had a history of coughing out of streaks of blood occasionally with a history of orthopnoea. Past history revealed joint pain during childhood mainly involving the large joints of lower limb, migratory in nature with associated swelling that got relieved on taking medications. On examination BP was 100/70 mmHg, pulse was regular, rhythmic with radio-radial and radio-femoral delay, Loud S1 with mid diastolic rumbling murmur with pre systolic accentuation on auscultation. ECG showed normal sinus rhythm with features of P-mitrale wave and normal QRS complexes. Transthoracic Echocardiography (TTE) revealed features of very severe mitral stenosis with thickened rheumatic mitral leaflets with a mitral valve area (MVA) of 0.9 sq-cm on planimetry and 1.1 sq-cm with pressure half time (PHT) method. The Mean Gradient (MG) across mitral valve (MV) was 14 mmHg. The patient had severe Tricuspid Regurgitation (TR) with a Pulmonary artery systolic pressure (PASP) of 72 mmHg. Transeosophageal Echocardiography (TOE) showed no presence of clot and a clear atrial appendage. The patient was taken for Balloon Mitral Valvotomy (BMV). After septal puncture, coiled wire was introduced into the left atrium followed by introduction of BMV balloon through the wire. After diagnostic catheterization, balloon valvotomy was attempted. However inflation of the balloon was not proper and an abnormal pattern of inflation was seen. Normally during balloon valvotomy, when the balloon catheter, properly aligned with the orifice, fails to cross the mitral valve, the distal balloon size is gradually reduced until its size is accommodated by the mitral orifice. In extreme instances, the catheter balloon, even when uninflated, is checked at the mitral valve. This finding is termed term “balloon impasse, which reflects a resistance caused by severe obstructive subvalvular lesions. This balloon compression is a reliable indication of severe subvalvular lesions and is used to supplement assessment by transthoracic and transesophageal echocardiography which oftenly underestimate the subvalvular disease severity.
 Awards Nomination
Awards Nomination