PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical Image - International Journal of Clinical & Medical Images (2015) Volume 2, Issue 1

Author(s): Fiona Kiely* and Feargal Twomey
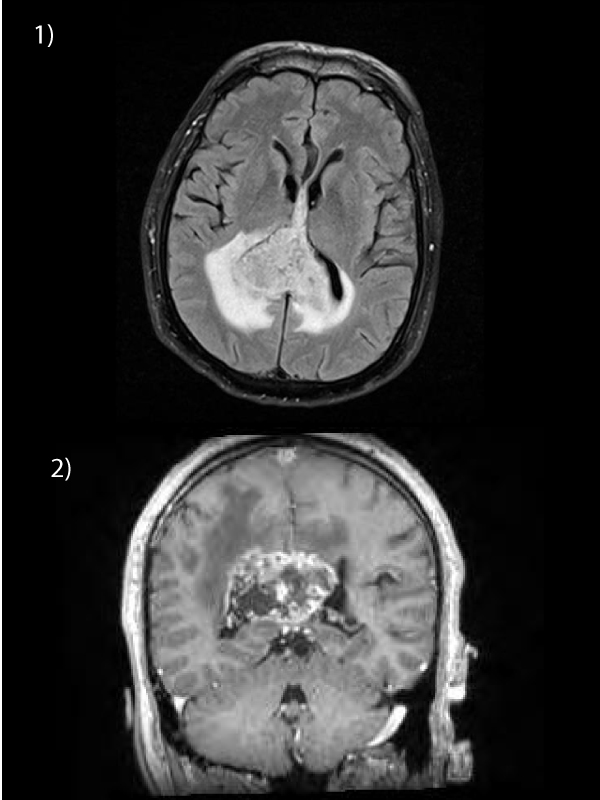
61 year old male presented with headache, nausea, vomiting, disorientation and ataxia. MRI brain revealed a heterogenous solitary mass suggestive of glioblastoma multiforme involving the splenium of the corpus callosum and crossing the midline, measuring 5.4 cm in transverse, 3.6 cm in antero-posterior, 3.3 cm in craniocaudal dimensions (Figures 1 and 2). Surrounding peritumoural edema was evident. Glioblastoma multiforme (WHO grade IV) was subsequently confirmed on biopsy and deemed inoperable by the neurosurgical team. The patient’s performance status precluded palliative chemotherapy. He was referred to the specialist palliative care inpatient unit to facilitate the planned ten fractions of palliative whole brain radiotherapy in conjunction with steroid therapy. Unfortunately his condition deteriorated further and he was unable to complete the planned protocol. Glioblastoma multiforme is the most common primary intra-axial malignancy, accounting for 12-15% of all intracranial neoplasms. It generally originates in the cerebral white matter and spreads along the corpus callosum in a “butterfly” pattern to the opposite side. The corpus callosum is divided into rostrum, genu, body, isthmus, and posteriorly, the splenium. The fibres in the splenium connect posterior parietal, medial occipital, and medial temporal cortexes. The splenium is primarily affected in this case and represents the least common are of callosal involvement (10%). Prognosis is poor. The median survival time from the time of diagnosis without any treatment is 3-6 months, but with treatment survival of 1-2 years is common. Increasing age (>60 years of age), abnormal brain function, or significant disabilities carry a worse prognostic risk.
 Awards Nomination
Awards Nomination