PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical Image - International Journal of Clinical & Medical Images (2014) Volume 1, Issue 7

Author(s): Ikeda M, Kataoka H, Marutani A and Ueno S
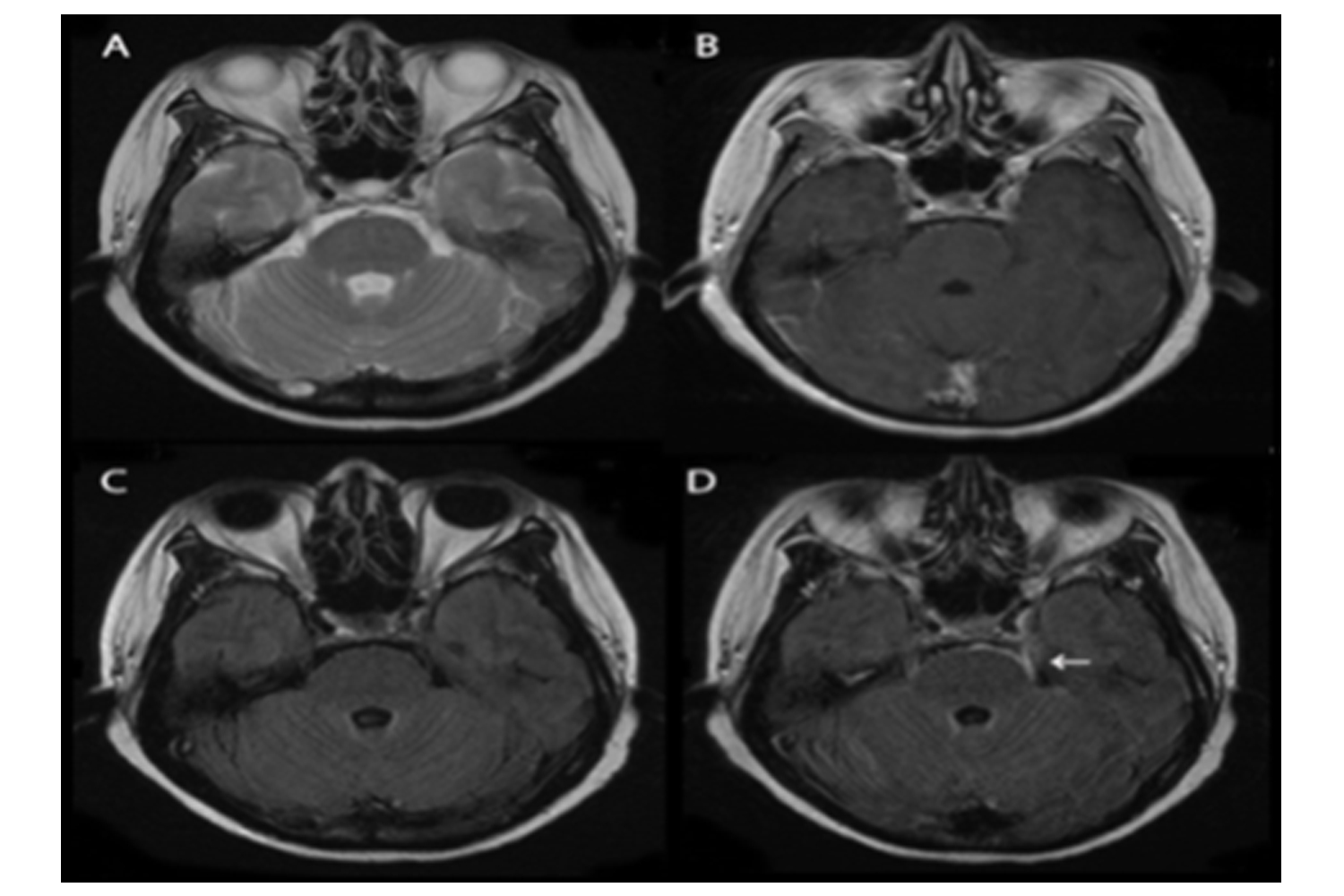
A woman in her early 50 s presented with headache, dizziness, and a high fever. Lumbar puncture showed an initial pressure of 210 mmHg, with 313 white cells/mm3 (90% polymorphonuclear leukocytes), a protein concentration of 198 mg/dl, and a glucose concentration of 74 mg/dl (serum glucose concentration, 199 mg/dl). The consciousness was clear, with meningeal and cerebellar signs. Cerebrospinal fluid (CSF) culture confirmed nocardia resistant to trimethoprim/sulfamethoxazole. The patient underwent 1.5-T magnetic resonance imaging (MRI) (Magnetom Sonata A.G., Siemens, Erlangen, Germany), using turbo spinecho sequences for T2-weighted images (T2WI) (TR 4000 ms; TE 91 ms), T1-weighted images (T1WI) (TR 492 ms; TE 9.4 ms), and fluid-attenuated inversion recovery (FLAIR) images (TR 10000 ms; TE 125 ms). Cranial MRI showed a ring-enhancing abscess and acute infarcts in the left cerebellum and medulla. Enlarged ventricles and some areas of leptomeningeal enhancement were evident. After the injection of gadolinium diethylenetriamine pentaacetic acid (Gd-DTPA 0.1 mmol/kg), contrast T1WI (TR 492 ms; TE 9.4 ms) and subsequent contrast FLAIR images (TR 10000 ms; TE 125 ms) were obtained. Enhancements of the leptomeninges were more apparent on contrast FLAIR images (panel d; arrow) than on contrast T1WI images (panel b). High signal intensity in the same lesions on contrast FLAIR images was more evident than that on non-contrast FLAIR images (panel c). Increased high signal intensity of the same lesion was absent on T2WI images (panel a). Contrast FLAIR images are especially useful for the detection of meningeal lesions that border the cerebrospinal fluid (CSF) [1].
 Awards Nomination
Awards Nomination