PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2020) Volume 7, Issue 6

Author(s): Najlae Lrhorfi*, Hasnae Moslih, Hounayda Jerguigue, Rachida Latib, Youssef Omor
Cortical laminar necrosis corresponds to an ischemic neuronal reorganization associated with a glial reaction and a laminar deposition of lipid-rich macrophages, the first case of which was described is in 1990 in a patient with hypoxic encephalopathy. It is a specific type of cortical infarction, which typically develops as a result of generalized hypoxia rather than focal vascular involvement. Oxygen or glucose deficiency, hypoglycemia, status epilepticus, stroke, or less commonly immunosuppressive therapy and polychimiotherapy have been attributed as the underlying cause of cortical laminar necrosis. Neurons in the cortex are much more metabolically active than glial cells or the adjacent white matter. In addition, the entire cortex is not at risk. There is a selective vulnerability of certain layers of the cerebral cortex (cortical layers 3, 5 and 6) to metabolic deficit.
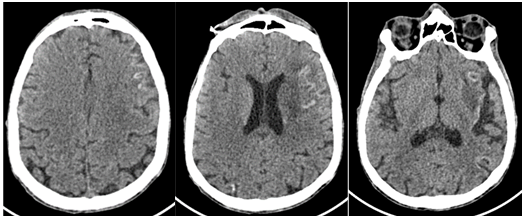
Ischemic changes appear 48 hours after the anoxic injury, while the glial reaction and the deposition of macrophages begin a few weeks later. Appearances of cortical laminar necrosis on CT can be subtle, appearing as gyriform changes in attenuation affecting more frequently the junctional areas, both hypodense and hyperdense depending on timing. Cortical hyperdensity, is observed after 2 weeks and will generally persist up to 6 months, gyral enhancement will also be noted, indicating a disruption of the blood-brain barrier (Figure 1).
 Awards Nomination
Awards Nomination