PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2015) Volume 2, Issue 10

Author(s): Hafeez Ul Hassan Virk*and Ali Raza Ghani
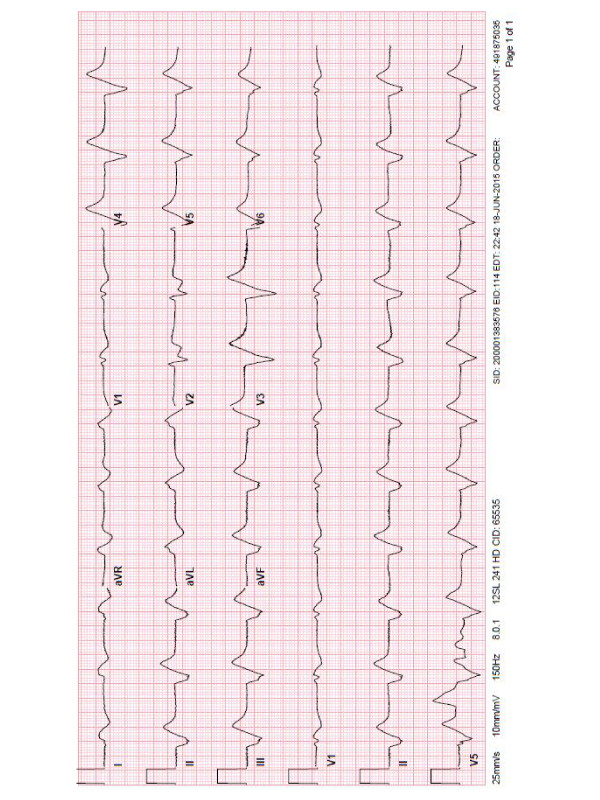
A 64-year old man with systolic heart failure and on chronic dose of digoxin, chronic kidney disease stage 3, was brought to ED after 2 episodes of syncope. He was hypotensive to 84/57 mm of Hg. The physical examination was unremarkable, but he was lethargic and feeling nauseated. EKG showed a regular rhythm, with a widened QRS complex in a sine-wave configuration with no visible P waves. The T waves were fused with the widened QRS complexes (Figure 1) to form the sine-wave pattern, concerning for severe hyperkalemia. The patient’s serum potassium level was 9.4 mmol per liter. Following medications were administered in ED; Calcium Gluconate, Digoxin immune Fab, insulin therapy, followed by urgent hemodialysis. Serial EKGs showed progressive narrowing of the QRS complex. On day 3 of admission, EKG revealed atrial fibrillation with slow ventricular response and left bundle-branch pattern (Figure 2).
Hyperkalemia destabilizes the cardiac membrane leading to electrocardiographic changes, initially with peaked T waves and PR prolongation. Severe elevations in potassium level results in loss of P wave and QRS widening, with sine-wave pattern observed in this case. It can lead to malignant arrhythmias if not treated promptly. At the time of discharge, digoxin was discontinued and follow-up in outpatient showed reversible ischemia on nuclear stress test.
 Awards Nomination
Awards Nomination