PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2021) Volume 8, Issue 4

Author(s): Anza Zahid, Derek R Johnson, Samantha J. Caron, and Sani H Kizilbash
Clinical Image
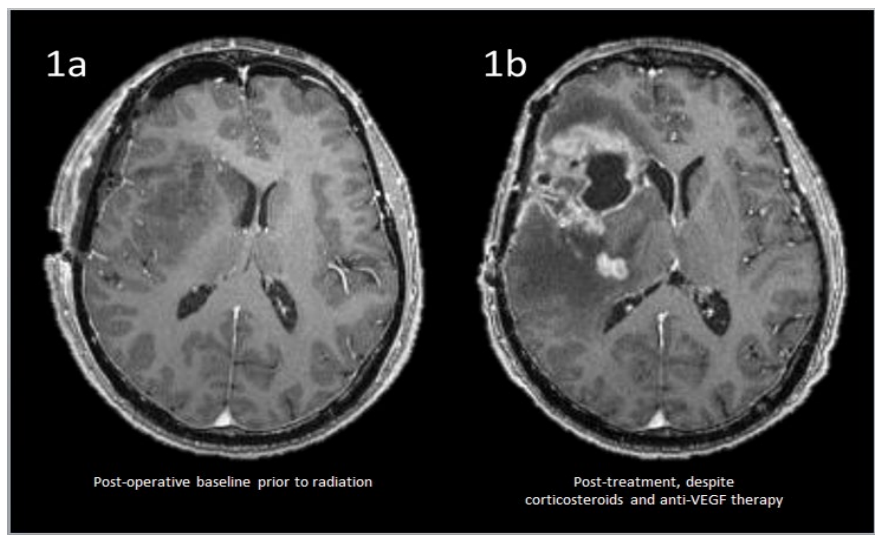
We present a 62-year-old male with IDH wild type, MGMT promoter unmethylated glioblastoma. After craniotomy and resection of the tumor, he was enrolled on a clinical trial involving treatment with radiation therapy, alternating electrical fields, and immunotherapy including both nivolumab and an IDO inhibitor [1]. A T1-weighted post-gadolinium axial MR image of the brain prior to radiation is shown in Figure 1a. During radiation, he developed severe headaches which prompted imaging. MRI brain revealed a significant interval increase in the size of the confluent heterogeneously enhancing mass involving the right basal ganglia, right frontal lobe, right temporal lobe, and a significant interval increase in confluent T2 and FLAIR hyperintensity. Under assumption of pseudoprogresssion, corticosteroids and bevacizumab were initiated leading to symptomatic resolution. MRI performed one month post radiation initially revealed transient significant interval radiographic improvement. However, subsequent imaging (three months post-radiation) revealed worsening enhancement on T1-weighted post gadolinium image (Figure 1b) and worsening vasogenic edema despite ongoing corticosteroids and bevacizumab therapy. Additionally, new abnormal T2/ FLAIR signal involving the right optic tract and optic chiasm was observed (not shown). A subtotal surgical resection of the enhancing mass-like lesion was performed to debulk the mass and establish a definitive histological diagnosis. Histopathology demonstrated cerebral neocortex and subcortical white matter with extensive therapy related changes, including vascular hyalinization, macrophages infiltrating astrocytoma, compatible with residual foci of patient’s previously diagnosed IDH-wild type glioblastoma. Pseudoprogression is a transient MRI pattern mimicking tumor progression, typically observed soon after chemo radiotherapy as a consequence of glioblastoma therapy [2]. Recent studies have shown pseudoprogression with atypical features in 20% of patients on nivolumab [3]. While recognition of pseudoprogression remains a diagnostic challenge, early consideration and histopathological confirmation can help prevent premature therapy cessation of efficacious immunotherapeutic agents and improve understanding of these therapies in patients with atypical imaging patterns [4,5].
 Awards Nomination
Awards Nomination