PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2016) Volume 3, Issue 1

Author(s): Rahul Vasudev, Upamanyu Rampal, Kunal Patel and Mahesh Bikkina
Image 1: Carotid ultrasound showing complete occlusion of internal carotid artery.
Image 2: Carotid ultrasound showing complete occlusion of internal carotid artery.
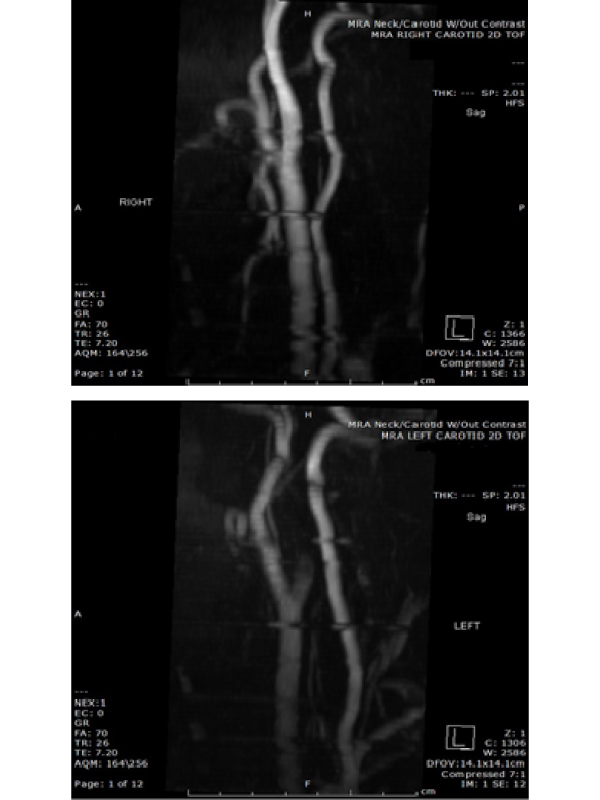
Image 3a: Magnetic resonance angiogram showing complete occlusion of internal carotid artery on left side (panel A); compare to right side (panel B).
Image 3b: Magnetic resonance angiogram showing complete occlusion of internal carotid artery on left side (panel A); compare to right side (panel B)
This is a 24-year-old Caucasian male with past medical history of intravenous drug abuse, hypertension, cardiomyopathy, endstage renal disease on hemodialysis 3 times a week (through AV fistula) was brought by the EMS after he was found by his mother lying on the floor drowsy. After further questioning in ER he complained of weakness in the right side of his body including the right upper limb and lower limb, he denied having any headaches, nausea or vomiting. On examination he was young cachectic male in moderate distress and febrile with a temperature of 102.3; Pupils were equal, round, reactive to light and accommodation.
Neurologic exam showed strength was 1/5 right upper and lower extremity and normal strength on left side. He also had a facial droop to the left side. On cardiovascular examination S1, S2 were heard with 3/4 diastolic murmur in the left parasternal region and decreased breath sounds in the bilateral lower lung bases. Neurology team was called and patient was taken for CT head which did not show any acute hemorrhage. Given the history physical findings and preliminary labs patient was admitted for Infective endocarditis causing septic emboli and stroke. Tran’s esophageal echocardiography confirmed the diagnosis with aortic
 Awards Nomination
Awards Nomination