PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical Image - International Journal of Clinical & Medical Images (2014) Volume 1, Issue 8

Author(s): Luis Mieiro
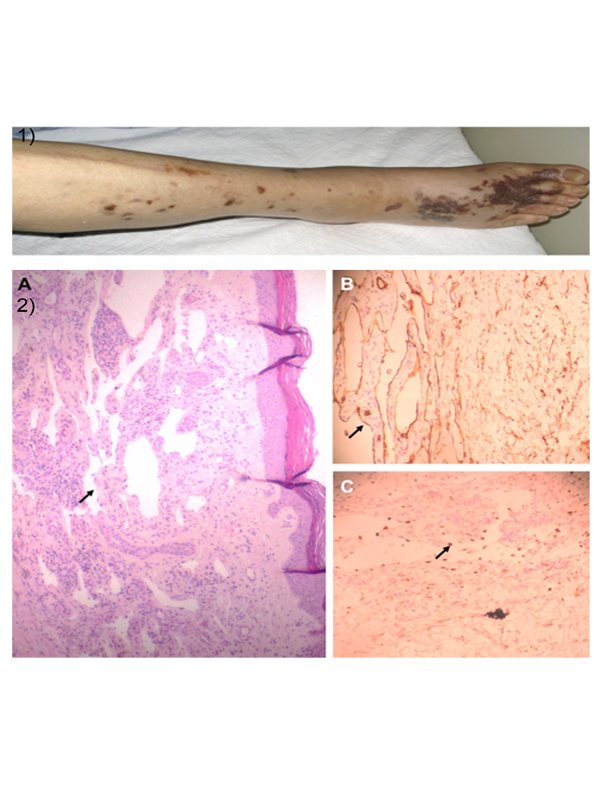
84-year old Caucasian male presents with tracheobronchitis. Known past medical history of hypertension and recurrent lower respiratory tract infections. On observation, remarkable sarcopenia and patchy nodular brownish-bluish cutaneous lesions on his right foot and leg (Figure 1) consistent with classic type Kaposi’s sarcoma (KS). Histology confirmed diagnosis (Figure 2). The patient was anti-Human Herpes Virus (HHV) 8 positive and anti-Human Immunodeficiency Virus (HIV) 1/2 negative. Whole body computerized tomography scan, upper gastrointestinal (GI) endoscopy and bronchial fibroscopy showed no organ spread of the disease. KS is a malignant tumor of endothelial lymph cells affecting most frequently skin, GI and respiratory tracts. There are 4 described types of KS: classic, presenting most often in middle-aged to elderly Mediterranean males; epidemic, associated to HIV infection; related to immunosuppressive therapy; and endemic, most commonly in sub-Saharan Africans. HHV8 infection has been implicated in KS pathogenesis. Sarcopenia is a marker of frailty and may contribute to an impaired immune response in older adults, allowing infections to develop in otherwise immunocompetent individuals. Therefore, classic type KS is the most frequent type in frail elderly males.Treatment should be considered on an individual basis and according to the spread of the disease and its impact on multiple organs. Figure 1: Sarcopenia and patchy nodular brownish-bluish cutaneous lesions on right leg Figure 2: A – Haematoxylin & eosin staining (x40) – Spindle cell proliferation of endothelial cells forming sinuous vascular spaces (arrow); B – Immunohistochemistry (x100) – Lesional cells positive to the non-specific endothelial marker CD34 (arrow); C – Immunohistochemistry (x100) – Lesional cells positive to antibody to HHV8 latent nuclear antigen 1 (arrow).
 Awards Nomination
Awards Nomination