PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2024) Volume 11, Issue 1

Author(s): Arshad Ali*
Department of Cardiology, All India Institute of Medical Sciences, New Delhi 110029, India
*Corresponding Author:
Arshad Ali
Department of Cardiology
All India Institute of Medical Sciences
New Delhi 110029, India
E-mail: drarshadcardio@gmail.com
Received: 01 January 2023, Manuscript No. ijcmi-24-124818; Editor assigned: 03 January 2023, Pre QC No. P-124818; Reviewed: 17 January 2023, QC No. Q-124818; Revised: 23 January 2024, Manuscript No. R- 124818; Published: 31 January 2024, DOI:10.4172/2376-0249.1000934
Citation: Ali A. (2024) LV Clot in Post PCI Post VT Ablated Patient with Severe LV Systolic Dysfunction. Int J Clin Med Imaging 11: 934.
Copyright: © 2024 Ali A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
67-year-old man with a past medical history of insulin-dependent diabetes and hypertension. He reported an acute onset central chest pain while using the restroom, with no initial symptoms.
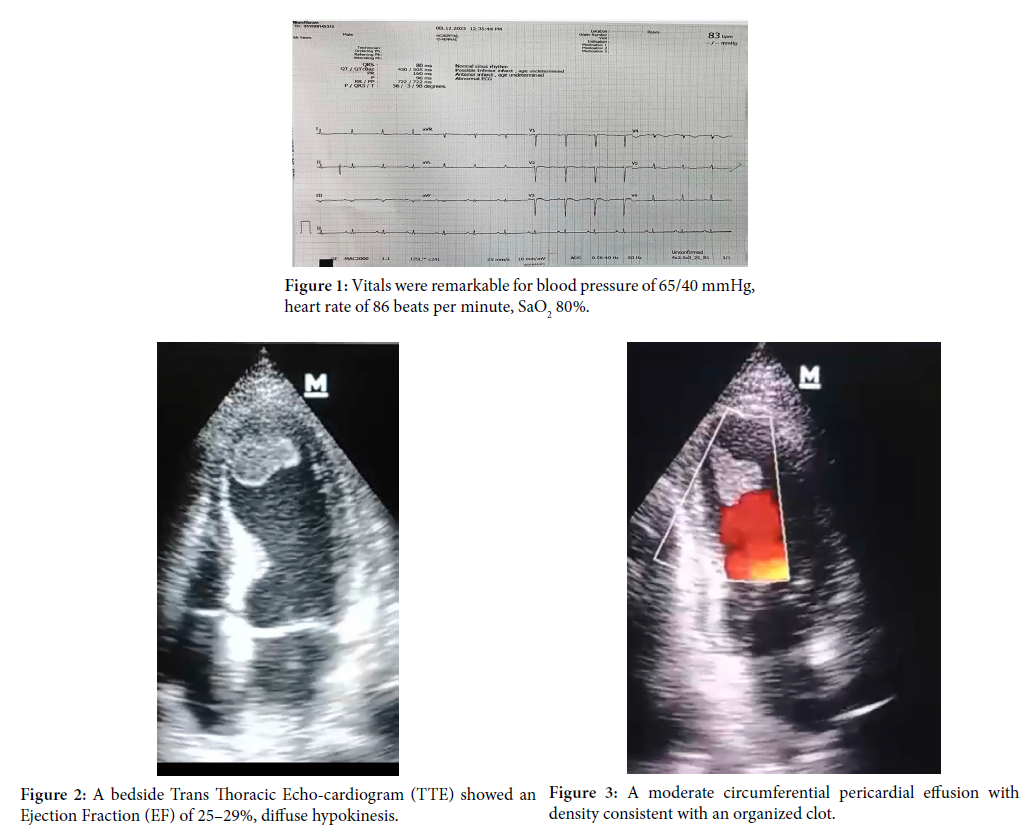
Upon arrival to the Emergency Department (ED), although initially hypertensive, he suddenly became hypotensive and reported feeling back pain. His vitals were remarkable for blood pressure of 65/40 mmHg, heart rate of 86 beats per minute, SaO2 80% (Figure 1). He was intubated and put to mechanical ventilator support. He underwent emergency CAG which revealed CAD TVD and primary PCI to LAD (infarct related artery). Post operatively he had persistent VT with hemodynamic compromise and refractory to medical management. In view of Polymorphic vt, ablation rfa of apical septal region was also done.
He was discharged and went home after 1 month of hospitalisation and had to undergo tracheostomy.
He again presented with class IV dyspnoea after 1 month. His physical examination was remarkable for visible and palpable double systolic apical impulse in the fifth intercostal space of the left midclavicular line and pericardial rub, with the first component representing the normal apical outward movement and the second the bulging of the aneurysm during peak ventricular pressure later in systole.
EKG showed diffuse QS in anterior leads and T wav changes in the inferior and lateral leads. A bedside Trans Thoracic Echo-cardiogram (TTE) showed an Ejection Fraction (EF) of 25–29%, diffuse hypokinesis, and a moderate circumferential pericardial effusion with density consistent with an organized clot (Figure 2 and Figure 3).
He was managed with oral anticoagulation (apixaban), antifailure and antiischemics medications and is on regular follow up [1,2].
Hypertension; Trans thoracic echo-cardiogram; Hemodynamic
None.
[1] Reed SC, Dhir N and Widmer RJ (2022). Optimal cardiovascular medical therapy: Current guidelines and new developments. Proc Bayl Univ Med Cent 35: 636–642.
Google Scholar, Crossref, Indexed at
[2] De Caterina R, Liga R and Boden WE (2022). Myocardial revascularization in ischaemic cardiomyopathy: Routine practice vs. scientific evidence. Eur Heart J 43: 387–390.
Google Scholar, Crossref, Indexed at
 Awards Nomination
Awards Nomination