PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2020) Volume 7, Issue 12

Author(s): Yahya Hsaini*, Jamal Mounach and Amal Satte
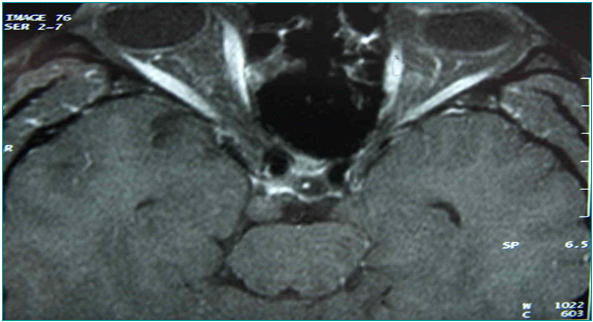
A previously healthy 36-year-old man was presented with a 6-month history of intermittent vertigo, chest tightness, and episodes of unconsciousness followed by postictal amnesia. The frequency of generalized seizures was two times a month. Symptoms were enriched in the last month by a binocular diplopia. Clinical examination found a global paralysis of the right third cranial nerve (III) with eye pain. There was no other neurologic deficit or pyramidal syndrome. Electroencephalogram (EEG) showed right temporal epileptic paroxysmal abnormalities. Cranial magnetic resonance imaging (MRI) revealed heterogeneous parasellar lesion, popcorn like on T1 and T2-weighted sequences, and hypointense on gradient echo sequences (T2*), no enhancing after administration of Gadolinium, extended to the medial temporal lobe. Cerebral angiography, cerebrospinal fluid, tumor, inflammatory, and immunological markers were normal. The diagnosis of parasellar cavernoma was established. Its location although unusual, correlated perfectly with mesiotemporal seizures and the common oculomotor nerve involvement in this case. Seizures were controlled with carbamazepin, and our patient was proposed for management of his cavernoma by gamma knife (Figures 1-3).
 Awards Nomination
Awards Nomination