PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2023) Volume 10, Issue 3

Author(s): Shanthi Mariapan*, Sangaran Gopal, Ruchi Negi, Bernardine Macrina and Tan YL
Hospital Shah Alam, Shah Alam, Selangor, Malaysia
Received: 13 March 2023, Manuscript No. ijcmi-23-91424; Editor assigned: 14 March 2023, Pre QC No. P-91424; Reviewed: 28 March 2023, QC No. Q-91424; Revised: 03 April 2023, Manuscript No. R-91424; Published: 10 April 2023, DOI: 10.4172/2376-0249.1000884
Citation: Mariapan S, Gopal S, Tan YL, Macrina B and Negi R. (2023) Paediatric Adhesive Bowel Obstruction: A Comment on Complication in Congenital Atresia and its Sequelae. Int J Clin Med Imaging 10:884.
Copyright: © 2023 Mariapan S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Causes of congenital gut atresia is polyhydramnions, malrotation and prematurity apart from genetic reasons as a resultant from in utero insult. The insult starts at a mesenteric blood supply, which gets impaired at a particular portion, causing fetal bowel reabsorbtion in utero, leaving behind a blind proximal and distal end of the bowel with a mesentery defect between the ends. Distally located atresia usually presents with delayed symptoms compared to proximal ones. Here is a commentary article on paediatric adhesive bowel obstruction: a comment on complications in congenital atresia and its sequelae.
Congenital atresia; Polyhydramnions; Malrotation
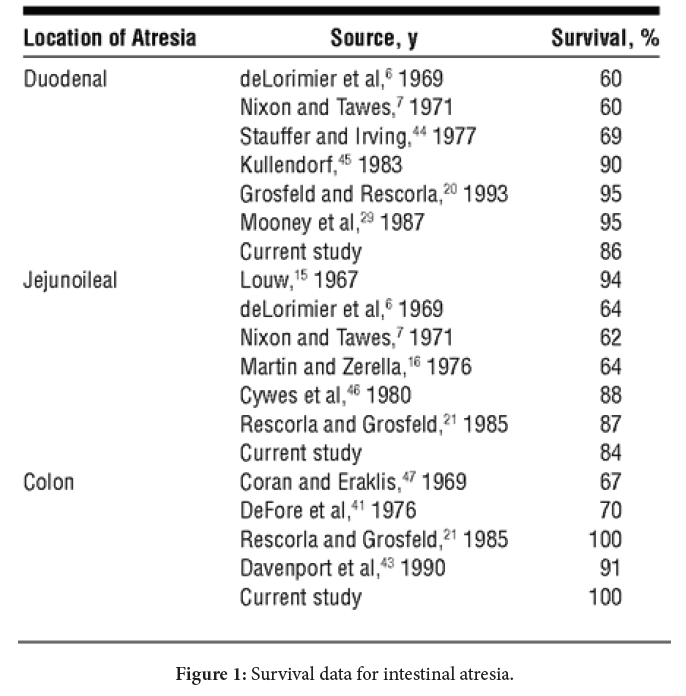
Mr A, 19 year old with underlying ileal atresia and currently admitted for adhesion. The case was clear cut resection and anastamosis with no graft. In 2019, relaparatomy and adhesiolysis. The diagnosis being intestinal obstruction secondary to adhesion as noted from CT scan done pre operatively- predominantly at the left hypochondrium. Patient presented with symptoms of vomiting for 4 days since discharged- food and bilious vomiting. 3 days later, still unable to tolerate orally – vomiting, nil by mouth for 2 days, abdomen distended, subjecting him for second CT abdomen with oral contrast. In summary, the adhesions may have been due to secondary infections, as it wasn’t at the site of resection. Here is an evaluation in graphical form of the survival data for intestinal atresia (Figure 1).
The survival rate for infants with intestinal atresia has remained relatively stable for the last 2 decades. The major obstacle to a successful outcome continuous to be ultrashort bowel syndrome and TPN related liver diseases. Refinements in small bowel transplantation and advances in science of immunology, should reduce the current high complication rate and improve graft and patient survival [1,2].
Scenario 1: A 48 hour newborn presents with bilous vomiting and a distended stomach was taken to the operation room.
Q: During surgery there is an obvious point of obstruction from ileal atresia and dilatation of the proximal end. The surgical technique that will reduce the bowel obstruction after surgery?
A: Historically, Jejunoileal Atresia with blind ends have high mortality due to functional obstruction from defective peristalsis after direct anastomosis of proximal and distal blind ends. The defective peristalsis and the mucosal necrosis of the blind ends seen in some cases of Jejunoileal Atresia are a result of vascular insufficiency. It has been postulated that the damage done to the blind ends is not enough to cause the death of the areas, but being close to the infarcted part of the bowel, a conclusion can be drawn that these areas are left with insufficient blood supply. Therefore, resection of the dilated proximal blind end and the proximal part of the distal atretic end in Jejunoileal Atresia has been reported with better functional outcomes.
Scenario 2: A 5 day old infant presents to the emergency department following multiple episodes of emesis after attempted feeds, dehydration lethargy and failure to thrive.
Q: A review of prenatal ultrasounds and obstretrics history reveals that the pregnancy was complicated by polyhydramnions. Emergent exploratory laparotomy as planned. On entering the abdomen multiple areas of jejunoileal atresia are seen with less than 25 cm of normal small bowel segment. What is the next step in the management of this patients?
A: The prognosis of Jejunoileal Atresia depends on the presence of short bowel syndrome (SBS) with an intestinal length of less than 25cm, requiring long-term parenteral nutrition. Jejunalileal atresia is responsible for about 10% of intestinal failure and the two most popular bowel lengthening procedures are serial transverse enteroplasty procedure (STEP) and longitudinal intestinal lengthening procedure (LILT).
Operative correction of colonic atresia has been modified over the years. Recent studies recommended resection and primary anastomosis as a reasonable treatment option regardless of the location of the colon atresia. In short bowel syndrome, early use of growth factor to maximise intestinal adaptation, administration of growth hormone to grow the bowel and nutritional modifications may improve the status.
No conflict of interest.
[1] Dalla Vecchia LK, Grosfeld JL, West KW, Rescorla FJ and Scherer LR, et al. (1998) Intestinal atresia and stenosis: A 25-year experience with 277 cases. Arch Surg 133: 490-497.
Google Scholar, Crossref, Indexed at
 Awards Nomination
Awards Nomination