PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Medical Image - International Journal of Clinical & Medical Images (2017) Volume 4, Issue 1

Author(s): Liao PH and Chen HY
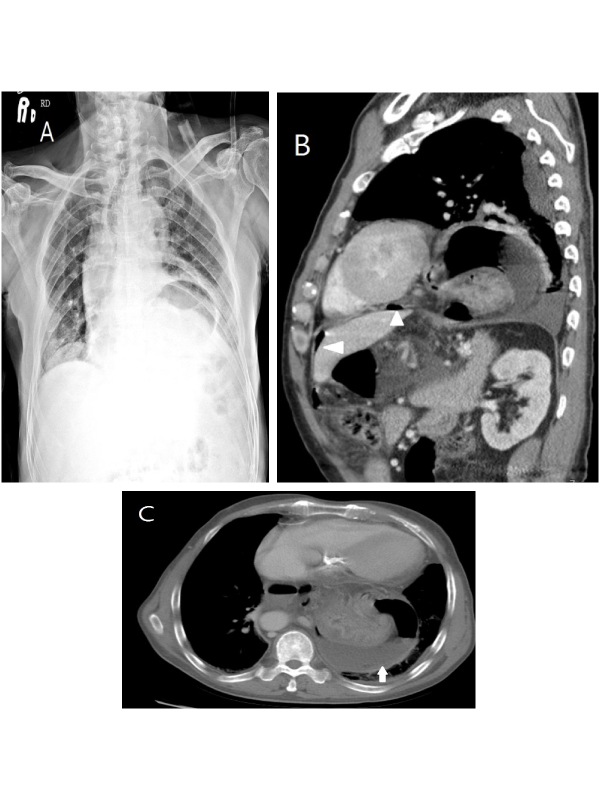
Clinical Imaging; An 81 year male came to our emergency department presenting with dyspnea and chest pain. The chest pain got worse on breathing and radiation to the epigastria. Past medical history included hiatus hernia and hypertension. His blood pressure was 88/63 mmHg, pulse rate 107 per minute. Abdominal examination revealed epigastria tenderness with voluntary guarding. Initial blood tests were all within normal limits. Chest X-ray revealed hiatal hernia with gas distension of the stomach (Figure 1A). Abdominal X-ray showed no diagnostic features. The abdomen CT reveals upper abdomen pneumoperitoneum in the periportal space and hernia sac (Figure 1B), moderate amount of ascites are also noted suspect gastric juice leakage (Figure 1C), indicating perforated gastric ulcer. He was taken for emergent exploratory laparotomy immediately .The right posterior wall fundus of gastric ulcer perforation 2 × 2 cm and upper gastric incarceration hiatal hernia were noted. The hiatal hernia repair and perforated ulcer repair were done. The patient recovered smoothly and was discharged 3 weeks later. Perforated gastric ulcer in an Incarcerated hiatal hernia is rare and the diagnosis is challenge. CT is the gold standard diagnostics and early surgery intervention reduces mortality and consequent complication.
 Awards Nomination
Awards Nomination