PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2022) Volume 9, Issue 5

Author(s): Edward Heydon* and Matthew Anstey
Received: 03 May, 2022, Manuscript No. ijcmi-22-56080; Editor assigned: 04 May, 2022, PreQC No. P-56080; Reviewed: 18 May, 2022, QC No. Q-56080; Revised: 23 May, 2022, Manuscript No. R-56080; Published: 28 May, 2022, DOI: 10.4172/2376-0249.1000829
Clinical-Medical Image
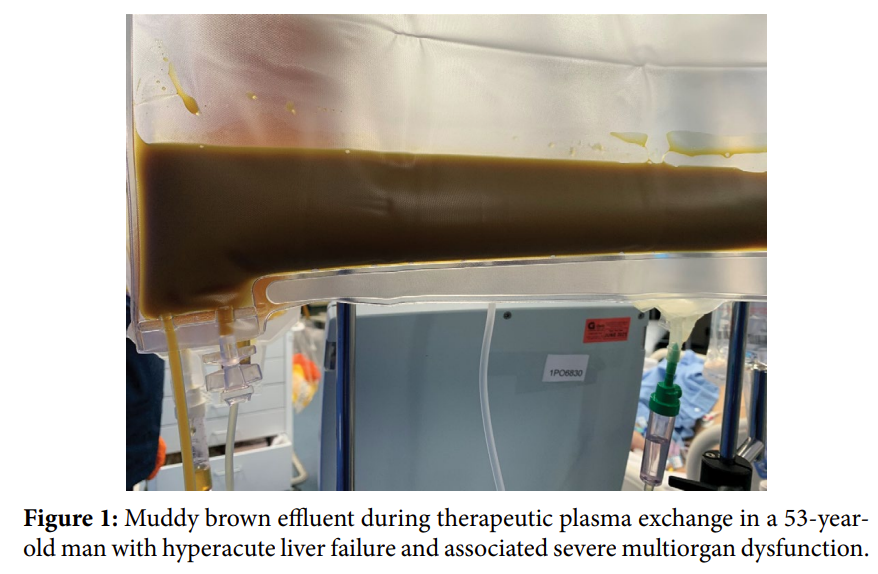
A 53-year-old man was admitted to our Intensive Care Unit (ICU) with hyperacute liver failure and associated severe multiorgan dysfunction. He had a bilirubin of 330 micromol/L, an International Normalised Ratio (INR) >10, and a lactate of 12.1 mmol/L. His Acute Physiology and Chronic Health Evaluation (APACHE) II Score on admission was 24. As an ICU with expertise in liver failure and transplantation, we often use continuous veno-venous haemodiafiltration (CVVHDF) for fulminant liver failure, but due to diagnostic uncertainty and multiple abnormalities in this case, Therapeutic Plasma Exchange (TPE) was chosen as an “artificial liver technique”. Plasma is normally clear and straw-coloured, but our patient’s plasma effluent was unusual in colour (Figure 1) [1]. Discolouration can suggest an underlying pathological or physiological process, a drug effect, and/or a complication of the plasmapheresis procedure itself [2]. Our patient was icteric, had evidence of haemolysis, and was hypertriglyceridaemic. In isolation, each of these conditions may cause an altered appearance of plasma; bright yellow, reddish and milky white discolouration’s respectively. The combination of these pathologies in our patient likely resulted in the muddy brown effluent. Despite the severity of presentation, the effluent cleared over several days and he survived, being discharged from hospital 56 days after presentation.
Keywords: Critical care; Acute liver failure; Therapeutic plasma exchange
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributions
EH and MA wrote the manuscript.
References
[1] Kirk FL, Bandhlish A, Arora, V, and Brown, CH (2014) The colour of plasma. Can J Anaesth 61: 209-210.
Google Scholar Crossref Indexed at
[2] Szczeklik W, Wawrzycka-Adamczyk K, Wludarczyk, Sega A, and Nowak-Kózka I, et al. (2013) Complications in patients treated with plasmapheresis in the intensive care unit. Anaesthesiol Intensive Ther, 45: 119-123.
Google Scholar Crossref Indexed at
 Awards Nomination
Awards Nomination