PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2019) Volume 6, Issue 4

Author(s): Ben Jmaa Hela*, Dammak Aiman, Fourati Kais, Mhiri Fatma, Elleuch Nizar, Masmoudi Sayda and Frikha Imed
Clinical-Medical images
Celiac artery aneurysm is a quite uncommon vascular lesion, accounting for 5.1% of all splanchnic artery aneurysms. In contrast to true aneurysms, with feature distension of all three layers of the arterial wall, so-called false aneurysms or pseudoaneurysms result from a breach of the inner-wall layers, resulting in bulging of the adventitial layer. False aneurysms have a higher risk to be ruptured. Rupture is a devastating presentation, with reported mortality rates ranging from 25% to 70%. The aneurysm may rupture into the peritoneal cavity, retro peritoneum, or thorax. Because of its rarity, no strong consensus concerning indications for intervention of asymptomatic celiac artery aneurysm exists in the literature. Treatment depends on the aneurysm’s size, presentation, and location. The risk of rupture of 15-22 mm diameter celiac artery aneurysms is 5%; in contrast, the risk of rupture in >30 mm diameter aneurysms is 50%-70%. In general, treatment is considered for asymptomatic patients when the aneurysm is larger than 20 mm in diameter.
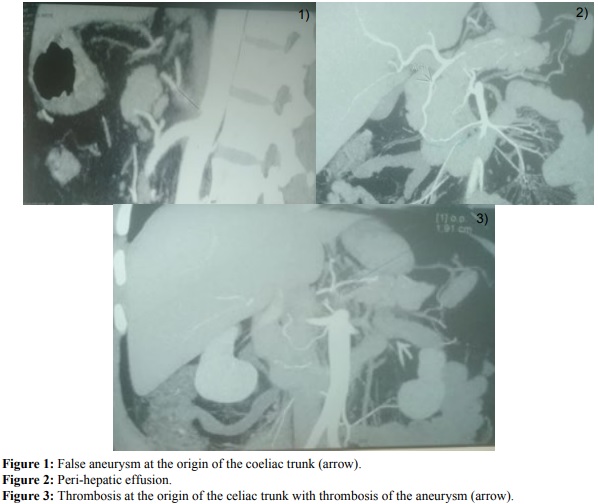
A 48-year-old man had been a victim of a traffic Accident (a nasty car accident) and was transferred to the emergency department. At the initial exsamination, he was aware and hemodynamically stable. The abdominal examination revealed an epigastria pain. The CT scan showed a false aneurysm at the origin of the coeliac trunk 13 mm with hematic infiltration retro peritoneal, low peri-hepatic effusion and complex acetabula fracture. Clinical, biological and radiological supervising was proposed as the patient was steady, becoming less symptomatic at the abdominal stage during hospitalization with blood pressure (BP) around 13/7, a pulse between 90 and 110 bpm, a hemoglobin level checked several times between 9 and 10 g/l. A control scanner made at the hospitalization showed no extension of the false aneurysm. Patient was discharged from hospital after a favorable clinical evolution, and then was reviewed at the consultation after a week. A control CT scan showed a complete thrombosis at the origin of the celiac trunk extended about 2 cm with permeability of these terminal branches from the gastro duodenal artery which diameter was increased.
 Awards Nomination
Awards Nomination