PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2014) Volume 1, Issue 4

Author(s): Int J Clin Med Imaging 2014
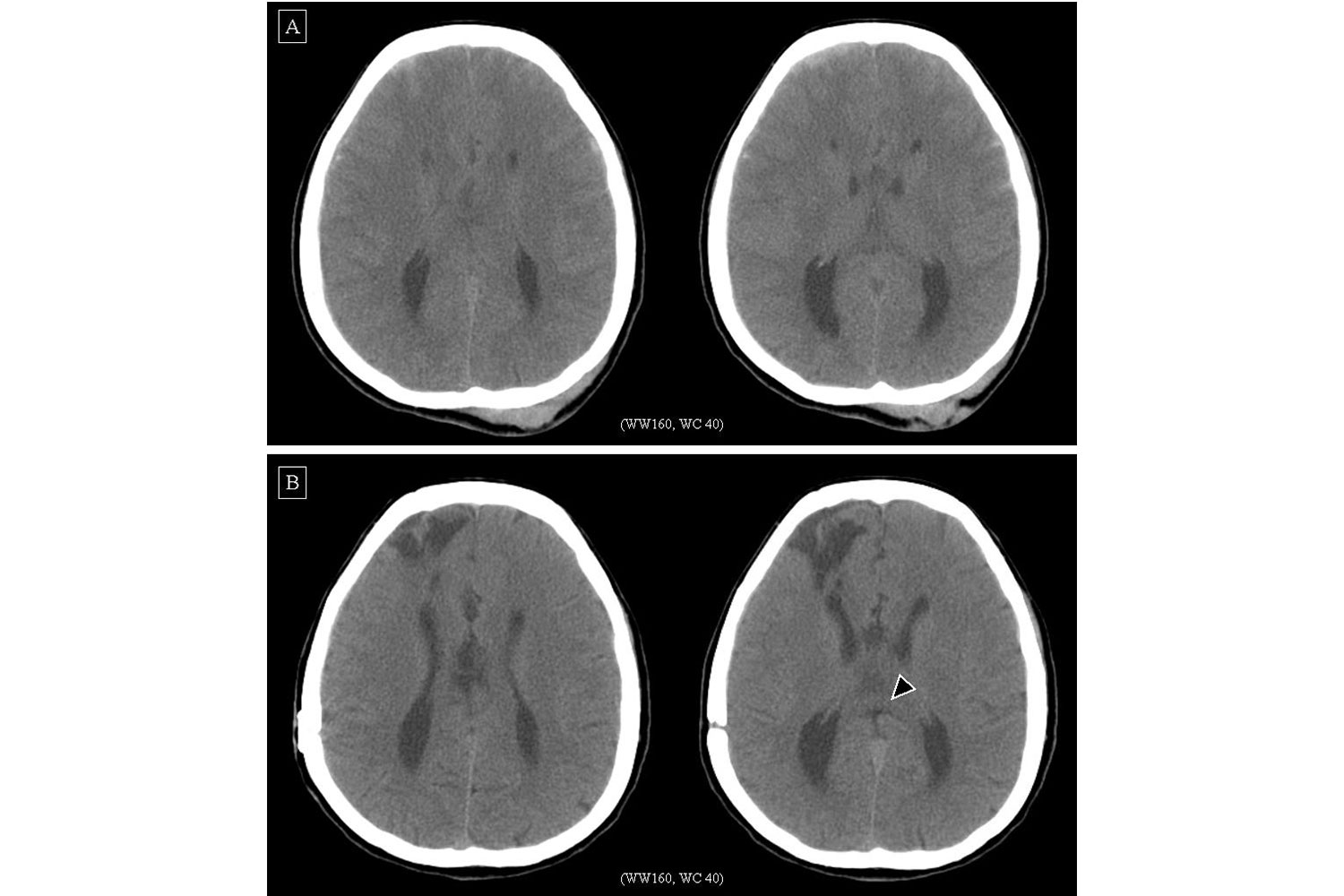
A 27-year-old female magazine editor with Turner’s syndrome did not have any neuropsychiatric disease or other systemic disease. She was sent to our hospital because of head trauma at a traffic accident. The Glasgow Coma Scale was E3V3M6, and computed tomography (CT) showed subarachnoid space hemorrhage, subdural hematoma, skull fracture and subgaleal hematoma; besides, widely near-parallel spaced lateral ventricles and teardrop-shaped dilatation of their posterior trigones (colpocephaly) were noted (Figure A). Craniotomy and removal of epidural hematoma, subdural hematoma, and intracerebral hemorrhage were recommended. After surgery, she was sent to the intense care unit, where intracranial pressure and partial brain oxygenation were monitored. One week later, the Glasgow Coma Scale was E4V5M6, and she was transferred to the common ward. On the 14th hospitalized day, she was discharged at stable condition. Four months later, computed tomography demonstrated right frontallobe encephalomalacia, and craniectomy defect at right frontotemporoparietal bone; besides, widely near-parallel spaced lateral ventricles and teardrop-shaped dilatation of their posterior trigones (colpocephaly) were still noted (Figure B), and splenium of corpus callosum were identified (Figure B, filled arrow-head). Corpus callosum is a great transverse commisure connecting both cerebral hemispheres. Between eight and 20 gestation weeks, it develops primarily from anterior to posterior with the genu forming first, then the anterior body, posterior body, and splenium. Between 18 and 20 gestation weeks, the rostrum finally forms [1] . An earlier insult, occuring before 12 gestation weeks, would cause incomplete formation of corpus callosum precursors, and result in agenesis (total absence). An insult slightly later, occurring between 12 and 20 gestation weeks, would result in hypogenesis (partial agenesis) with preservation of a genu or a genu and anterior portion of body. An insult to the brain after 18~20 gestation weeks may cause degeneration of the crossing fibers and would result in hypoplasia, which is fully formed, but is thinner than the same age of the other normal persons, just as our case patient [1,2]. The prevalence of corpus callosum corpus callosum maldevelopment was 1.8 per 10,000 live births [3]. Among them, 17.3% have chromosomal abnormalities, in which 37.6% (41 of 109) are aneuploidy, including Patau syndrome (trisomy 13), Edward syndrome (trisomy 18), Down syndrome (trisomy 21), Klinefelter (45, XXY) and Turner syndrome (45, X); in addition, 49.5% (54 of 109) have central nervous system (CNS) malformations, including cortical malformation, posterior fossa abnormality (cerebellar vermis or hemisphere abnormality, brainstem abnormality, Chiari malformation), encephalocele, and spinal cord abnormality [3]. Based on the accompanying CNS or other non-CNS malformations, Szabó et al classified them into four groups [4]: (I) isolated corpus callosum corpus callosum maldevelopment, just as our case patient, (II) corpus callosum corpus callosum maldevelopment associated with other CNS abnormalities, (III) corpus callosum corpus callosum maldevelopment associated with both CNS and non-CNS abnormalities, and (IV) corpus callosum corpus callosum maldevelopment associated only with non-CNS abnormalities. Corpus callosum corpus callosum maldevelopment may be symptomatic depending on the type of the associated anomaly [4]. This usually results in developmental defects, seizures, psychomotor or mental retardation [1,5]. However, some can be asymptomatic and is incidentally found by either neuroimaging or autopsy [5]. Pneumoencephalography, cerebral angiography, CT and sonography are useful tool for evaluation. CT has been most widely used, but it is difficult to identify a milder form. Magnetic resonance imaging could show all variations of callosal anomalies exquisitely [1]. In our case patient, the corpus callosum maldevelopment has not been noted till a traffic accident happened to her and an emergent CT was recommended. Furthermore, on axial TI magnetic resonance imaging or axial CT, colpocephaly is an associated ventricular morphology [6], and the near-parallel ventricular arrangement looks like a formula one car seen from above, with the widely spaced anterior horns representing the anterior wheeling tires, and the dilated posterior horns representing the posterior driving tires so is called “racing car sign” [7]. For an infant patient, presence of congenital heart disease seems to be an important prognostic factor [5]; and for a senior one, the prognosis would be better if without other associated anomalies, but the prognosis varies if with other associated anomalies, depending on the type of the associated anomaly [5]. In our case patient, that corpus callosum hypoplasia did not influence her intelligence, and she was healthy except Turner’s syndrome. If it were not the head trauma after the traffic accident, the corpus callosum hypoplasia would not be noted. Afterwards, she should be regularly followed for the sequela of head trauma and brain injury rather than corpus callosum hypoplasia.
 Awards Nomination
Awards Nomination