PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2014) Volume 1, Issue 10

Author(s): Yuh-Ming Chang*
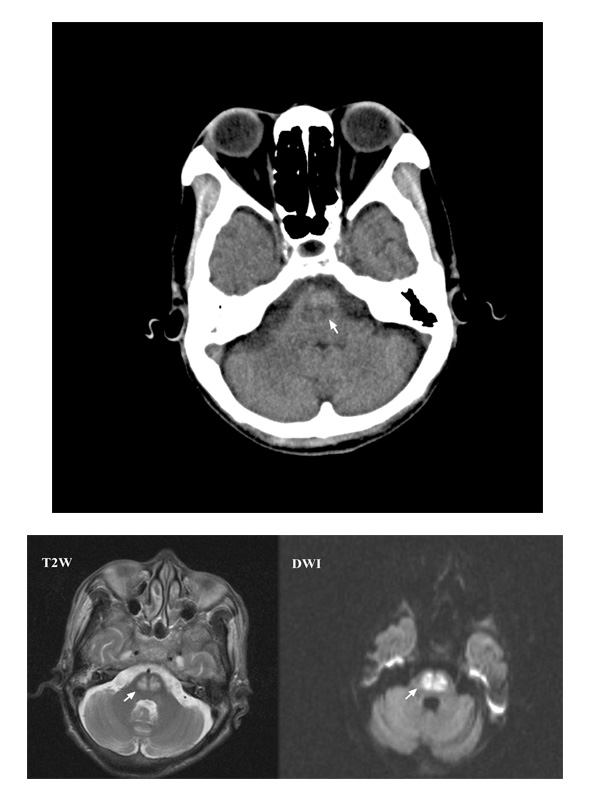
A 56-year-old woman with a poorly controlled type-2 diabetes mellitus presented with progressive dysarthria, dysphagia, and general weakness for 5 days. On admission, she had 36.8°C temperature, 111/53 mmHg blood pressure, 59 beats/min heart rate, and 20 breaths/min respiratory rate. On neurological examination, she was lethargic with pseudobulbar palsy and quadriparesis. Laboratory studies revealed blood glucose was 545 mg/dL, HbA1c 17.3%, sodium 137 mEq/L, blood urea nitrogen 19 mg/dL, and calculated serum osmolality was 311 mOsm/kg. Emergent computed tomography of brain showed a central pontine hypodensity
(Figure 1). A follow-up Magnetic Resonance Imaging (MRI) of brain showed a central pontine hyperintensity with peripheral sparing on T2-Weighted (T2W) and Diffusion-Weighted (DW) images (Figure 2), consistent with acute Central Pontine Myelinolysis (CPM). After insulin infusion, her hyperglycemia was corrected and her neurological deficit improved gradually
after 1 month.
CPM is an acute noninflammatory demyelinating condition involving the central pons. Hyperosmotic stress result from rapid
 Awards Nomination
Awards Nomination