PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2015) Volume 2, Issue 4

Author(s): Alex H Wong, Alexander KC Leung* and Benjamin Barankin
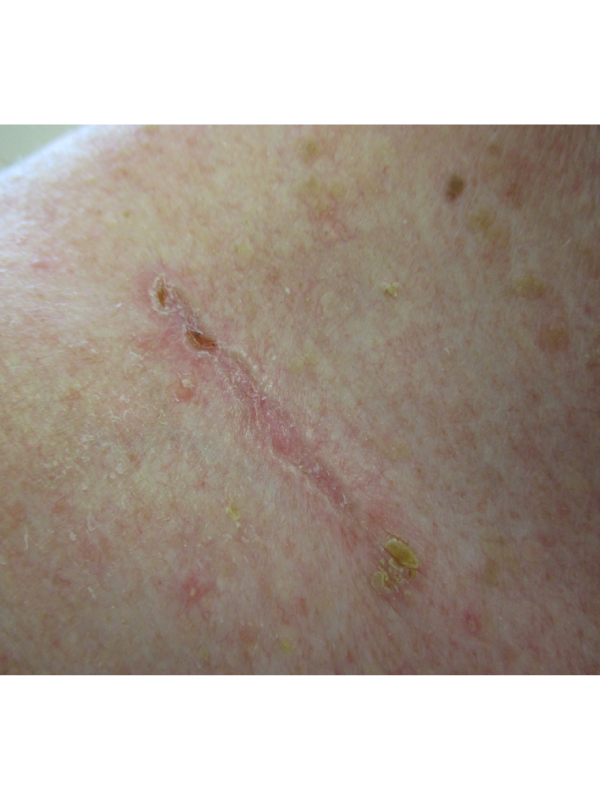
An 85-year-old Caucasian man presented with a slowly growing, asymptomatic, linear, scar-like lesion just above the right clavicle for almost four years. There was no history of weight loss or regional lymphadenopathy. He participated in many outdoor activities such as swimming when he was young. A punch biopsy of the lesion showed nests of basaloid cells arranged in elongated strands and embedded in a dense fibrous stoma, extending down from the epidermis into the deeper dermis. These features were consistent with a sclerosing basal cell carcinoma. Basal cell carcinoma (BCC) is generally defined as a locally invasive, slowly spreading tumor that rarely metastasizes, arising in the epidermis or hair follicles. The exact incidence is not known. In the UK, there were approximately 200,000 patients with BCCs treated surgically in 2010. This number does not include those treated by other means. The incidence increases with age, with a peak during the sixth to eight decades. The male to female ratio is approximately 1.5 to 2:1.
The greatest risk factor is chronic exposure to ultraviolet radiation as evidenced by a higher frequency of disease in sun-exposed areas. Other risk factors include fair skin color, history of blistering sunburns (particularly in childhood), freckles in childhood, ionizing radiation, indoor tanning exposure, arsenic exposure, immunosuppression, close relatives with skin cancers, and mutations in tumour suppressor genes such as p53 and patched homologue 1 (PTCH 1). BCCs are a heterogeneous group of tumors that based on their clinical morphology can be classified most commonly into the following subtypes: nodular BCC, superficial BCC, sclerosing BCC, infiltrative BCC, micronodular BCC, and pigmented BCC. Sclerosing BCC accounts for approximately 0.6% of all BCCs. It affects mainly the face as a depressed plaque or scar with illdefined borders. In fact, a sclerosing BCC is also called “cicatricial” or “morpheic” BCC for that reason.
he tumor is locally invasive and tends to extend into the dermis beyond the level where it is clinically visible or palpable. It can have an extensive subclinical spread, making complete excision difficult. Although sclerosing BCC rarely metastasizes, it carries a higher risk of local recurrence; periodic lifelong monitoring is advised to detect recurrence as well as to identify other skin cancers and precancers (i.e., actinic keratoses).
The requested URL was not found on this server.
Additionally, a 404 Not Found error was encountered while trying to use an ErrorDocument to handle the request.
 Awards Nomination
Awards Nomination