PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2015) Volume 2, Issue 7

Author(s): Clifford R*, Jones R, Mahapatra S, Vimalachandran D, Eardley N, Sheikh A
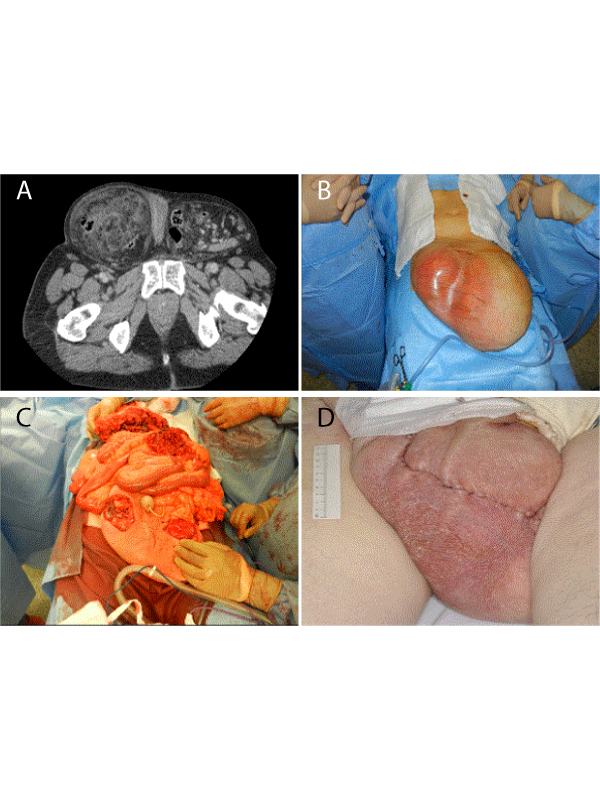
A 63 year old male with a long standing history of large bilateral inguino-scrotal herniae presented as an emergency with increasing scrotal pain, and raised inflammatory markers. CT abdomen/pelvis confirmed the presence of ischaemic bowel, with herniation from proximal jejunum to sigmoid colon. Following a multi-disciplinary approach and discussion with the patient regarding surgical intervention, a laparotomy and scrotal exploration was undertaken. A subtotal colectomy with end ileostomy formation was performed, along with scrotal skin reduction to allow full return of abdominal viscera to the abdominal cavity without the need for component separation. Surgical options described in the literature include a staged procedure using large breast expanders to create space in the peritoneal cavity, following which a laparotomy and return of abdominal viscera to the abdominal cavity is undertaken. In the emergency setting however bowel sacrifice and component separation are usually employed.
 Awards Nomination
Awards Nomination