PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Case Blog - International Journal of Clinical & Medical Images (2014) Volume 1, Issue 4

Author(s): Int J Clin Med Imaging 2014
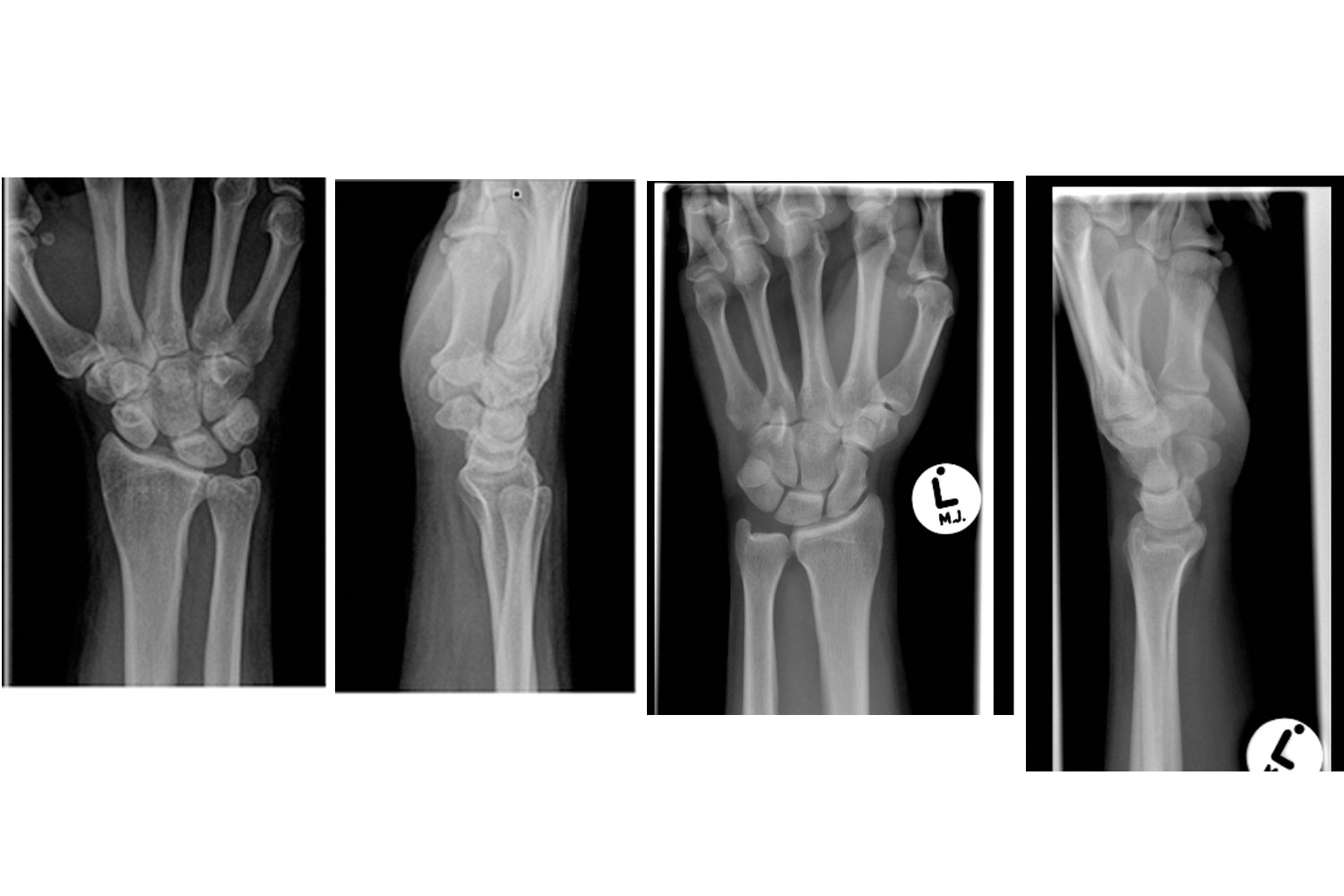
An otherwise fit and well 35 year old gentleman presented with a several month history of radial sided wrist pain after a fall onto an outstretched hand. Clinical examination revealed swelling and tenderness most pronounced dorsally just distal to Lister’s tubercle in the region of the scapholunate ligament. The range of movement in the wrist was mildly restricted globally. Specialised tests for the scapholunate ligament- the Kirk Watson scaphoid shift test and the scapholunate ballottement test were positive. Plain radiographs of the wrist were taken (Figures 1 and 2). They revealed the four typical radiological signs for scapholunate disruption. On the PA view- the “Terry-Thomas” sign caused by widening of the scapholunate space (normal, <3 mm), the cortical ring sign caused by the abnormally flexed scaphoid creating a double density, and an abnormally triangular shaped lunate. On the lateral view the scapholunate angle was greater than 70 degrees as the scaphoid flexes palmarly and the lunate tilts dorsally. This is known as a “DISI” deformity as it arises from Dorsal Intercalated Segmental Instability. These abnormalities are more apparent when compared to a normal wrist radiograph (Figures 3 and 4). The “Terry-Thomas” sign is generally the most readily distinguished abnormality on plain radiographs in this injury pattern. The sign is named after the famous British comic from the 1950’s who had a trademark gap between his two front teeth / frontal dental diastema. The patient failed a period of nonoperative treatment and went on to have delayed reconstruction of the scapholunate ligament via a modified Brunelli procedure and did well.
 Awards Nomination
Awards Nomination