PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical-Medical Image - International Journal of Clinical & Medical Images (2022) Volume 9, Issue 8

Author(s): Qiuyu Yu MM, Tingjuan Pang MM, Ge Sun MM, Mei Xian MD*
Obstetrics and Gynecology Center, The Second Hospital of Jilin University, Changchun 130022, P.R. China
Date of Submission: 24 August 2022, Manuscript No. ijcmi-22-73185; Editor assigned: 25 August 2022, Pre QC No. P-73185; Reviewed: 26 August 2022, QC No. Q-73185; Revised: 27 August 2022, Manuscript No. R-73185; Published: 31 August 2022, DOI: 10.4172/2376-0249.1000843
Citation: Qiuyu Yu, Tingjuan Pang, Ge Sun and Mei Xian. (2022) Type II Residual Horn Uterine Pregnancy Complicated with Unilateral Kidney Deficiency: A Case Report. Int J Clin Med Imaging 9:843.
Copyright: © 2022 Xian M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Reason: Stump pregnancy refers to a special ectopic pregnancy in which the fertilized egg implants, grows and develops in the stump uterus. The incidence is very low, and it is difficult to make a diagnosis in the first trimester. We report a case of an early stump uterine pregnancy complicated by ipsilateral renal absence for retrospective analysis and literature review.
Patient concern: A 22-year-old woman presented with 51 days of stopping menstruation. A hysteroscopic uterine pregnancy embryo resection was performed at a local hospital. The operation failed because the entrance to the left uterine cavity was not found. After completing the relevant examinations in our hospital, a diagnosis of unicornuate uterus with residual horn uterine pregnancy was made.
Intervention: The patient took oral mifepristone for two days and had no obvious symptoms of vaginal bleeding. A hysteroscopy was performed, but the passage of the left uterus was not explored. An open left stump hysterectomy was performed to remove the pregnancy and left salpingectomy.
Outcomes and lessons: After three months of follow-up, the patient recovered well. Therefore, once a stump uterine pregnancy is detected, surgical intervention is required. Early intervention and prompt treatment are essential to improve prognosis.
Uterus with residual horn; Pregnancy; Disease report; Literature review
HCG: Human Chorionic Gonadotropin; MRI: Magnetic Resonance Imaging; MTX: Methotrexate
The stump uterus pregnancy refers to the implantation, growth, development of the fertilized egg in the stump uterus. The incidence of stump uterus pregnancy is very low, only 176.000-1, 150.000.5 [1]. Pregnancy with stump uterus is rarely maintained to term, with many cases diagnosed only after pregnancy rupture, with an estimated maternal mortality rate of 0.5 percent [2]. According to related reports, it is precise because of its rarity and lack of experience in ultrasound diagnosis that it is difficult to make a diagnosis in the first trimester. Only 14% of cases are diagnosed before symptoms [3]. A residual horn that does not communicate with the unicornuate uterus is mainly found during cesarean section [4]. This delays the treatment and even has adverse consequences. This article reports a retrospective analysis of a patient with stump horn uterine pregnancy in our hospital in the first trimester-and a review of relevant literature to help the clinical diagnosis and treatment of this case.
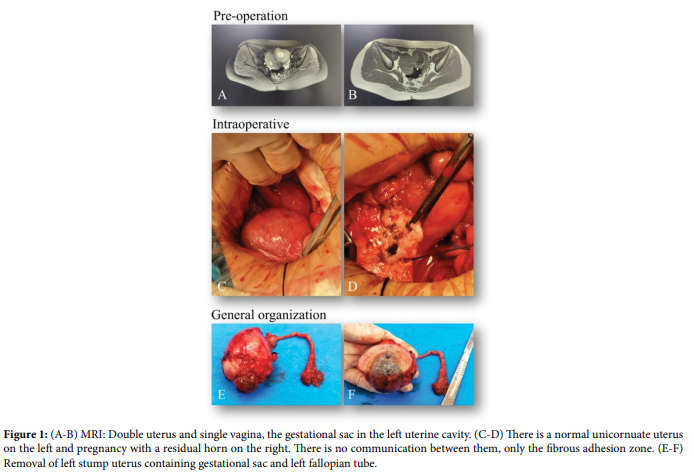
The patient, female, 22 years old, was admitted to our hospital on 2022-01-11 because of “51 days of menopause, requiring induced abortion”. History of present illness: The patient stopped menstruation for more than 30 days, took a urine pregnancy test (+) at home, and then went to the local hospital for gynecological ultrasonography. Lateral uterine entrance, the operation failed, so he was admitted to our hospital. Menstrual history: normal menstrual cycle, 14 7/30 days, a moderate amount, dysmenorrhea (+), relieved spontaneously, a blood clot (+), LMP: 2021-11- 21. Marriage and childbearing history: G4P2, one biochemical pregnancy, two cesarean sections. Gynecological examination: normal growth and development of vulva and vagina, free vagina, smooth surface of the cervix, repeated examination showed one vagina and one cervix; that two uterine bodies were palpable. Pain; the right uterus is posterior, normal size, without tenderness. No obvious abnormalities were palpated in the bi-adnexal area. Gynecological ultrasound shows: that two uteri can be detected in the pelvic cavity, the one on the left is slightly larger, such as 45-50 days of pregnancy, the size of the embryo sac is about 2.5×1.9cm in the uterus, and the echo of the yolk sac and fetal bud, and the bud can be seen in the uterus. It is about 0.5cm long can reach the heartbeat; the echo of the muscle layer is still uniform, the right side is generally large, the thickness of the intima is 0.9 cm, and the echo of the uterine wall is uniform. Ultrasound: Abnormal uterine morphology, double uterus? Intrauterine early pregnancy live foetus, please combine with clinical. Ultrasonography of the urinary system: no obvious renal tissue echo was detected in the left kidney area, the volume of the right kidney increased compensatory, and the left kidney was absent. Pelvic MRI: the double uterus and single vagina, left uterine cavity gestational sac. Bilateral endometrial thickening was considered a pregnancy response (Figure 1A and 1B). Blood progesterone: 21.00 ng/ mL. Blood Human Chorionic Gonadotropin (HCG): 125524.60 mlU/ ml. The patient was given oral mifepristone germicidal therapy, had no vaginal discharge and underwent hysteroscopy to confirm the diagnosis. Hysteroscopy showed that only one cervical orifice was observed to communicate with the left uterus, and there was no obvious connection between the two uteri. Through consultation and discussion of the general practitioner and the patient’s medical history examination, physical examination, and auxiliary examination: The patient’s previous second pregnancy was a good intrauterine pregnancy, and the patient reported that she had found a right unicornuate uterus with a left stump uterus during a cesarean section 6 years ago, while this pregnancy was left. There is only one cervix, and the two sides of the uterus do not seem to be connected. Only unilateral fallopian tube opening is seen during hysteroscopy, and the probe can only enter the right uterine cavity. Still, it cannot enter the left side, and oral mifepristone is used. There is no obvious sign of miscarriage after killing the embryo. To sum up, the diagnosis is considered as 1) Intrauterine early pregnancy 2) Uterine developmental malformation (single vagina and double uterus?) 3) Unicornuate uterus with residual horn uterus pregnancy 4) Congenital absence of left kidney. After communicating with patients and their families, an open left residual horn hysterectomy with pregnancy removal and left salpingectomy will be performed on 2022- 01-14. Intraoperative findings: double uterus, the left stump uterus is larger, and the uterus is located in the left front and communicates with the left fallopian tube and the left ovary. The right unicornuate uterus is normal and large and is connected with the right fallopian tube and ovary. The uterine cavity is connected, and the uterine body of the left residual horn does not have an obvious cervix. It is connected with the lower segment of the left wall of the unicornuate uterus with a muscular fibrous band. There was no obvious abnormality in the double appendage area (Figure 1C-1F). Intraoperative diagnosis: the right unicornuate uterus and left residual horn uterus pregnancy. Postoperative pathological report: (muscle wall and gestational sac), villi, decidua, and trophoblast cells were seen in the submitted tissue, consistent with pregnancy. (Left fallopian tube) Focal nests of Warthard cells with cystic degeneration. The patient’s blood HCG was re-examined after operation: 14772.57 mlU/ ml, and he recovered well and were discharged from the hospital. After follow-up, the patient’s blood HCG decreased to negative.
Pathogenesis
The female reproductive system originates from the Mullerian ducts, which fuse during embryonic development to form the fallopian tubes, uterus, and upper two-thirds of the vagina [5]. The stump uterus results from abnormal formation, fusion or resorption, and developmental failure of Miller’s ducts [6]. There is a close embryological relationship between the development of the urinary and reproductive organs, [7] and approximately 38% of patients have concurrent renal abnormalities such as unilateral renal agenesis, usually ipsilateral to the stump. [8] Cerekja A, et al. [5] also confirmed the link between the urinary tract and reproductive organ abnormalities, suggesting that it is essential to look for kidney abnormalities every time we diagnose uterine hypoplasia. The absence of the lateral kidney supports the diagnosis of the left stump uterus.
Pregnancy mechanism
The primary mechanism of non-communicating residual horn uterine pregnancy with unicornuate uterus may be intraperitoneal transfer through sperm or fertilized oocytes [9-11].
(1) The fertilized egg first travels from the contralateral fallopian tube to the abdominal cavity through the intraperitoneal cavity The fallopian tube on the side of the stump horn uterus, and then into the stump horn uterus and implantation growth and development.
(2) Sperm first travels from the contralateral fallopian tube through the abdominal cavity to the fallopian tube on the side of the stump horn uterus, combines with the oogonia to form a fertilized egg enters the stump horn uterus to implant and grow and develop.
Clinical manifestations
There is no specific symptom of stump uterine pregnancy, most of which are asymptomatic. Still, for non-communicating stump uterus with functional endometrium, if the blood flow in the stump is blocked, it may lead to ectopic pregnancy, Periodic or progressive dysmenorrhea, chronic pelvic pain, or menstrual disturbances [12-14]. It has been reported that approximately 50 percent of patients remain asymptomatic [15]. In this case, after a detailed medical history questioning, the patient said dysmenorrhea but no apparent progressive worsening.
Classification
According to the relationship between the stump uterus and the interior of the unicornuate uterus, the stump uterus can be divided into the following three types.
Type I: The stump uterus is solid, without cervix or uterine cavity, and only cellulose is connected to the unicornuate uterus.
Type II: The stump uterus has no cervix but has a uterine cavity and has normal endometrial tissue: 1) Type IIa: communicates with the medial side of the unicornuate uterus; 2) Type IIb: does not connect with the unicornuate uterus.
Type III: Contralateral unicornuate uterus without stump uterus [7,14].
However, the patient had four pregnancies according to the patient’s condition. The previous two pregnancies were all unicornuate uterine cavity pregnancies. This pregnancy was a stump uterus, so it was considered type II because there was normal endometrial tissue. Pregnancy is possible, but the uterine cavity of the unicornuate uterus is not connected. Therefore, the hysteroscopy in the local hospital was unsuccessful, and the opening was not seen during the operation. Consequently, it is necessary to stop the pregnancy in time to avoid uterine rupture.
Complications
Obstetric complications of stump uterine pregnancy with unicornuate uterus may include the following: spontaneous abortion, preterm labor, dysmenorrhea, endometriosis, intrauterine growth restriction, intraperitoneal hemorrhage, urologic dysplasia, and most severe of uterine rupture [16]. The total number of uterine ruptures occurred in 61% and 6% in the second and third trimesters of pregnancy [17]. Kaveh M, et al. reported a case of uterine rupture of a non-communicating stump horn misdiagnosed as intrauterine pregnancy at 14 weeks of gestation, and a patient with hemorrhagic shock underwent emergency resection of the stump horn [16] Similarly, Maninder, K et al. also reported a case of 11-week gestational rupture of the stump uterus leading to massive bleeding that was misdiagnosed as pregnancy with severe anemia [18]. So stump horn uterine pregnancy rupture can be the most potent and deadly complication. This may be due to hypoplasia of the myometrium, with reported rupture times ranging from 5 to 37 weeks, possibly depending on the strength of the myometrium, the thickness of the myometrium, and the distensibility of the muscle [19]. Zhang Y, et al. [17]. reported a case of a patient who was terminated by cesarean section with a newborn at 38 weeks of gestation. The patient was diagnosed with a stump uterus pregnancy and became pregnant four years later.
Auxiliary inspection
Ultrasound imaging has always been the first choice for the supplementary examination of stump uterine pregnancy. Still, the sensitivity is low, only about 26%, and decreases with the increase of gestational weeks. Tsafriret, et al. [17]. Proposed the following criteria for the ultrasonographic diagnosis of stump uterine pregnancy: (1) Pseudo-pattern of asymmetric bicornuate uterus. (2) There is no visual continuity around the gestational sac and uterine cervix. (3) There is uterine muscle tissue around the gestational sac. Typical placental hyperplasia with vascular hyperplasia may support the diagnosis. The diagnostic criteria proposed by Mavrelos D, et al. [20]. (1) The main body of the uterus has only one interstitial part of the fallopian tube; (2) a mobile gestational sac separated from the uterus and surrounded by myometrium. (3) Interconnected capillary pedicles between the gestational sac and the unicornuate uterus. Therefore, an initial diagnosis can be made by ultrasonography. Magnetic resonance imaging (MRI), as a non-invasive examination method, has great significance for the diagnosis and differential diagnosis of stump uterine pregnancy and has greater accuracy in diagnosing uterine malformations [17]. However, due to insufficient understanding of the residual horn uterus, ultrasound examination technology and MRI and other auxiliary examination methods are still unable to distinguish the size of the double uterus and the developmental relationship between the uterine cavity of the pregnant uterus and the cervix.
Differential diagnosis
Because most of the stump uterus and the unicornuate uterus have only a few fibrous bands adhering to each other, it is easy to be misdiagnosed as uterine fibroids or female ovarian tumors. It is necessary to ask the patient’s medical history in detail and combine it with its auxiliary examination. Pregnancy with a stump uterus needs to be differentiated from any other type of ectopic pregnancy, or intrauterine pregnancy with uterine malformation, such as twin uterine pregnancy, interstitial pregnancy, intra-abdominal pregnancy, etc. [21]. Both uterine bodies in a twin uterine pregnancy are continuous with their respective cervix and can often be delivered to term. Interstitial pregnancy is not separated from the uterus and is diagnosed by the adjoining uterine cavity and the ipsilateral interstitial duct of the gestational sac. Intra-abdominal pregnancies are mainly secondary to ectopic tubal rupture, usually located in the broad ligament and fixed deep in the pelvis, with poor mobility when palpated [20].
Treatment
Due to the potential risks of stump uterine pregnancy, when a stump uterus pregnancy is detected, early preventive surgery is recommended to remove the stump uterus and the attached fallopian tubes to prevent re-ectopic pregnancy and avoid the effects of retrograde menstruation and reduce dysmenorrhea [9]. Bleeding is a significant surgical risk when the stump of the uterus of pregnancy is removed because of the high blood flow to the pregnant uterus. Studies have found that local or systemic MTX injections can reduce the risk of bleeding during surgery followed by surgical resection [11]. Related literature studies have found that laparoscopic surgery is a feasible and safe method in the first trimester of stump uterine pregnancy [22]. Zhang NN, et al. [23]. Found that for accurate identification and management of type IIb uterine malformations, simultaneous hysteroscopy and laparoscopy is a practical and feasible method.
Pregnancy with a stump uterus is rare, and early diagnosis is difficult. Once the pregnancy ruptures, intra-abdominal hemorrhage can be lifethreatening. Therefore, if a stump uterus is found to be pregnant, surgical treatment is required to achieve early detection, early examination, early diagnosis, and early treatment to prevent severe complications and avoid adverse pregnancy outcomes.
Ethics approval and consent to participate
Not applicable
Consent for publication
Informed consent of the patients has been obtained for this article.
Availability of data and materials
Not applicable
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Not applicable
Investigation: Qiuyu Yu&Tingjuan Pang
Supervision: Ge Sun, Mei Xiang
Resources: Qiuyu Yu&Tingjuan Pang
Writing–original draft: Qiuyu Yu
Writing–review & editing: Qiuyu Yu
The authors are grateful to our department colleagues and the devotion of this patient, and the patient has signed the informed consent form.
[1] Dhanawat J, Pape J, Stuhlmann‐Laeisz C, Maass N and Freytag D et.al. (2021) Ectopic pregnancy in noncommunicating horn of unicornuate uterus: 3D‐ultrasound and primary laparoscopic management. Clin Case Rep 9: e04261.
Google Scholar, Crossref, Indexed at
[2] Yassin A, Munaza S and Mohammed A. (2019) Tale of rudimentary horn pregnancy: case reports and literature review. The Journal of Maternal-Fetal & Neonatal Medicine 32: 671-676.
Google Scholar, Crossref, Indexed at
[3] Walker C, Collins L, Pham A, George J and Johnson S. (2020) Avoiding the fatal misdiagnosis of pregnancy in a noncommunicating rudimentary horn using 3D transvaginal ultrasound. Journal of Clinical Ultrasound 48: 553-556.
Google Scholar, Crossref, Indexed at
[4] Mengistu K, Bobe T, Tilahun G, Kifle K, and Geleta D. (2020) Rudimentary horn pregnancy diagnosed after laparotomy. Case rep obstet gyne 5816487-5816487.
Google Scholar, Crossref, Indexed at
[5] Cerekja A, Dillon KC, Racanska E and Piazze J. (2011) Unicornuate uteri associated with contralateral renal agenesis and ovarian anomalies. J Turk Ger Gynecol Assoc 12: 189.
Google Scholar, Crossref, Indexed at
[6] Lefere M, De Vuysere S, De Bruecker Y, and Demeyere A. (2016) Unicornuate Uterus with Noncommunicating Cavitary Horn. J Belg Soc Radiol
Google Scholar, Crossref, Indexed at
[7] Makroum AAE-W, Abdelrazik MM and Hassan MSE-D. (2020) Minilaparotomy for Excision of a Functioning Noncommunicating Rudimentary Horn and Endometrioma in a Patient with Solitary Kidney: A case report. Gynecol Minim Invasive Ther 9: 91.
Google Scholar, Crossref, Indexed at
[8] Qamariya A and Chitra J. (2014) Pregnancy in the rudimentary uterine horn case report of an unusual presentation. Sultan Qaboos Univ Med J 14:e134-138.
Google Scholar, Crossref, Indexed at
[9] Dove CK, Harvey SM and Spalluto LB. (2018) Sonographic findings of early pregnancy in the rudimentary horn of a unicornuate uterus: A two case report. Clin Imaging, 47: 25-29.
Google Scholar, Crossref, Indexed at
[10] Bhagavath B, Ludwin A and Lindheim SR. (2020) Reunification of the unicornuate uterus and the remnant horn–proceed with caution!. Fertil Steril 114: 981-982.
Google Scholar, Crossref, Indexed at
[11] Ueda M, Ota K, Takahashi T, Suzuki S and Suzuki D et al. (2021) Successful pregnancy and term delivery after treatment of unicornuate uterus with non-communicating rudimentary horn pregnancy with local methotrexate injection followed by laparoscopic resection: a case report and literature review. BMC Pregnancy and Childbirth 21: 1-8.
Google Scholar, Crossref, Indexed at
[12] Nagshabandi ZK, Isaac B and Begum I. (2022) Unicornuate Uterus with Rudimentary Horn as a Rare Etiology of Secondary Dysmenorrhea: A Case Report. Dubai Med J 4: 326-329.
[13] Delic R. (2020) Pregnancy in a Unicornuate Uterus with Non-Communicating Rudimentary Horn: Diagnostic and Therapeutic Challenges. Acta Med Litu 27: 84-89.
Google Scholar, Crossref, Indexed at
[14] Pinto e Passos IdM and Britto RL. (2020) Diagnosis and treatment of müllerian malformations. Taiwan J Obstet Gynecol 59: 183-188.
Google Scholar, Crossref, Indexed at
[15] Yildirim D, Turkgeldi LS, Tekiner N, Seckin KD and Yucel B. (2017) A case of rudimentary horn pregnancy diagnosed after failed attempts at pregnancy termination. Niger J Clin Pract 20: 111-114.
Google Scholar, Crossref, Indexed at
[16] Hussain A, Jawaid H, Faisal N, Shah N and Kamal NS. (2018) Ruptured rudimentary horn pregnancy revealed on emergency laparotomy: a case of primigravida presenting in a developing country. Cureus 10.
[17] Zhang Y, Pang Y, Zhang X, Zhao Z, and Liu P. (2020) Full-term pregnancy in a rudimentary horn with a live fetus: a case report. Medicine 99.
Google Scholar, Crossref, Indexed at
[18] Ghotra Jr, M. K., Joshi, B., & Bhutani, S. (2021) Ruptured Rudimentary Horn Pregnancy: Delayed Diagnosis. Cureus 13.
Google Scholar, Crossref, Indexed at
[19] Parveen R. (2019) Detection and Management of Pregnancy in Rudimentary Horn of Uterus. J Coll Physicians Surg Pak 29: S70-S72.
Google Scholar, Crossref, Indexed at
[20] Mavrelos D, Sawyer E, Helmy S, Holland TK and Ben‐Nag J. (2007) Ultrasound diagnosis of ectopic pregnancy in the non‐communicating horn of a unicornuate uterus (cornual pregnancy). Ultrasound Obstet Gynecol 30: 765-770.
Google Scholar, Crossref, Indexed at
[21] Jomaa S, Ahmad A, and Adwan, D. (2021) Successful diagnosis and management of prerupture rudimentary horn pregnancy in the second trimester: a case report. Radiology Case Rep 16: 3068-3071.
Google Scholar, Crossref, Indexed at
[22] Chatziioannidou K, Fehlmann A, and Dubuisson J. (2020) Case report: Laparoscopic management of an ectopic pregnancy in a rudimentary non-communicating uterine horn. Frontiers in Surg 85.
Google Scholar, Crossref, Indexed at
[23] Zhang NN, Zuo N, Chen SL, Bi FF and Yang Q. (2022) Accurate identification and surgical correction of type IIb uterine malformation using synchronized hysteroscopy and laparoscopy.Fertil Steril 117: 232-233.
 Awards Nomination
Awards Nomination