PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical Image - International Journal of Clinical & Medical Images (2021) Volume 8, Issue 1

Author(s): Safaa Choayb*, Olaia Chalh, Nazik Allali, Latifa Chat and Siham Elhaddad
Clinical Image
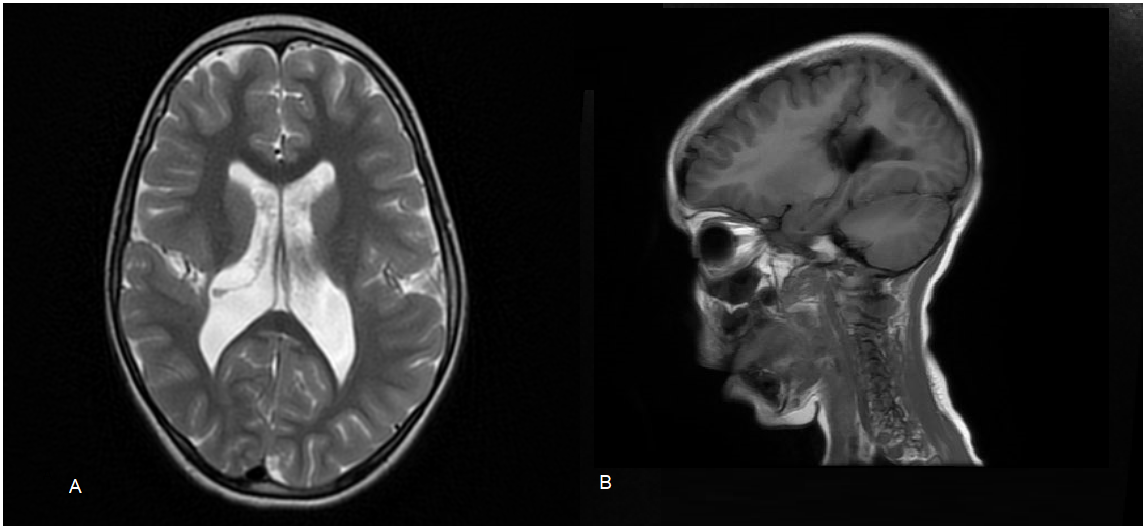
We present a case of a 4-year-old boy presenting seizures and developmental delay. A brain MRI showed a deep cleft in the right frontoparietal region. It was lined by grey matter that extends through the full thickness of the right cerebral mantle into the lateral ventricle body. These features were consistent with closed-lip schizencephaly.
Comment
Schizencephaly is a rare malformation of the central nervous system, secondary to neuronal migration defects occurring at the beginning of migrational events in the third month of gestation. It is characterized by a cleft extending from the ependymal surface of the brain to the pia mater. In type I or ‘closed-lip’ schizencephaly, the cleft is fused, without cerebrospinal fluid passage. In type II or ‘open- lip’ schizencephaly, the cleft extends from the cortical surface to the ventricle (pia to ependyma), without a connecting band of grey matter [1]. The exact cause of schizencephaly is unknown. It can be genetic by mutations in one of these four genes: EMX2, SIX3, SHH, and COL4A1 or non-genetic (young maternal age, infections such as cytomegalovirus (brain calcification may be present), warfarin use, toxin, trauma, and amniocentesis). The non-genetic causes involve a destructive process mediated by a vascular injury that causes impairment of the blood supply to the fetus. Symptoms of schizencephaly depend on the size of the lesion and whether if it is unilateral or bilateral. When the lesion is small and unilateral, the patient may present unilateral paralysis and mild or no intellectual disabilities; in contrast, larger bilateral hemisphere lesions usually present with quadriplegia and severe intellectual disabilities. Other signs and symptoms observed are global developmental delay, seizure, spasticity, and hypotonia [2]. MRI is the imaging modality of choice. The pathognomonic finding is the dysplastic grey matter lining the cleft, which differentiates schizencephaly from porencephaly (lined by gliotic white matter) [2]. Open-lip schizencephaly should also be differentiated from semi-lobar holoprosencephaly (can mimic bilateral open-lip schizencephaly) [2]. The cleft is often thickened by pachygyric or polymicrogyric cortex with heterotopia. Other associated abnormalities include hydrocephalus (in 50% of open- lipped schizencephaly), agenesis of the septum pellucidum (in 70% of cases), septo-optic dysplasia (in 10% to 25% of cases), and agenesis or hypoplasia of the corpus callosum (in 30% of schizencephalics) [1]. The therapeutic management consists of treating seizures and hydrocephalus (Figure 1).
Keywords: Schizencephaly; Type 1 schizencephaly; Closed-lip schizencephaly
 Awards Nomination
Awards Nomination