PHONE
+44-7482-878921
+44-7482-878921
2376-0249
Clinical Image - International Journal of Clinical & Medical Images (2014) Volume 1, Issue 4

Author(s): Int J Clin Med Imaging 2014
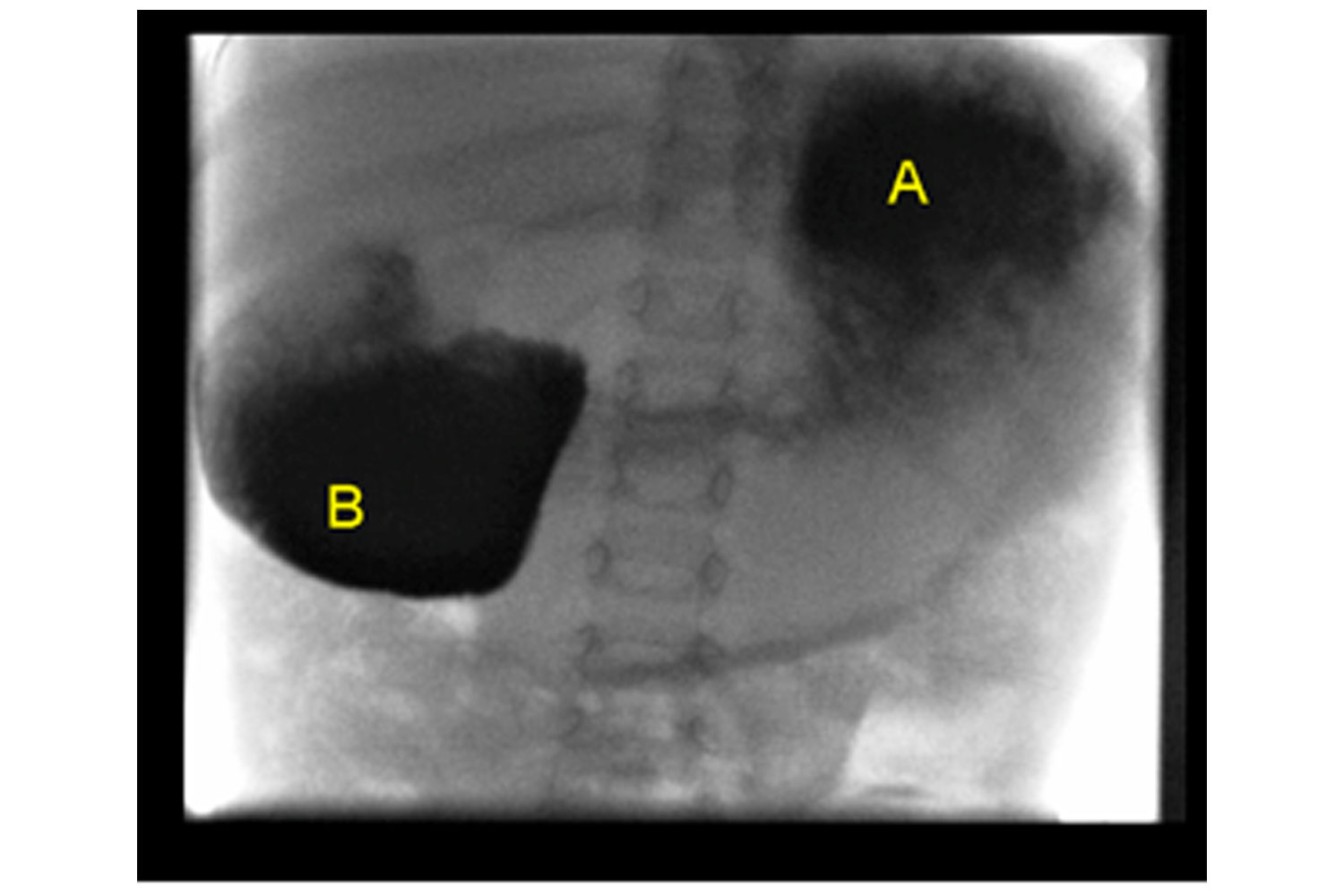
A 15 month old girl, born at term, developed bilious vomiting in the neonatal period. Upper gastrointestinal contrast study which was performed at a local paediatric centre, at age of 5 weeks, was unremarkable. She continued to have recurrent episodes of projectile vomiting, on average 8 times per day, with the interval between episodes being 2 weeks approximately. Bilious vomiting occurred as the episodes progressed. No history of temperatures, diarrhoea or constipation has been documented. Multiple admissions to a local paediatric centre have been required, with transient improvement being noticed following intravenous fluid therapy. At the age of 15 months, she was admitted to the tertiary centre with episode of projectile vomiting. Apart from mild dehydration, systemic examination was unremarkable. She was tracking below the 9th centile for weight. Further investigation including screening for metabolic disorders was reported normal. Although it was unremarkable at 5 weeks of age, upper gastrointestinal contrast study was considered and a duodenal web was diagnosed (Figure 1). Duodenal web which occurs due to defects in embryologic development usually presents in infancy [1] with symptoms of gastric outlet obstruction, such as vomiting. However it can present in adult [1, 2]. Our experience underlines the importance of considering congenital surgical causes in infants and children with prolonged recurrent vomiting, even if imaging was previously unremarkable. A= Barium demonstrates a grossly distended stomach containing fluid and debris. B= The first and proximal portion of the second part of the duodenum are grossly distended. There is vigorous peristalsis through the lower half of the second part of the duodenum noted in an attempt to pass contrast into the third part of the duodenum.
 Awards Nomination
Awards Nomination